Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited, Cambridge, MA, USA.
Projections Research Inc., Phoenixville, PA, USA.
Br J Clin Pharmacol. 2019 Nov;85(11):2568-2579. doi: 10.1111/bcp.14078. Epub 2019 Sep 4.
A population pharmacokinetic (PK) analysis was conducted to quantify the impact of patient-specific and concurrent medication factors on pevonedistat PK.
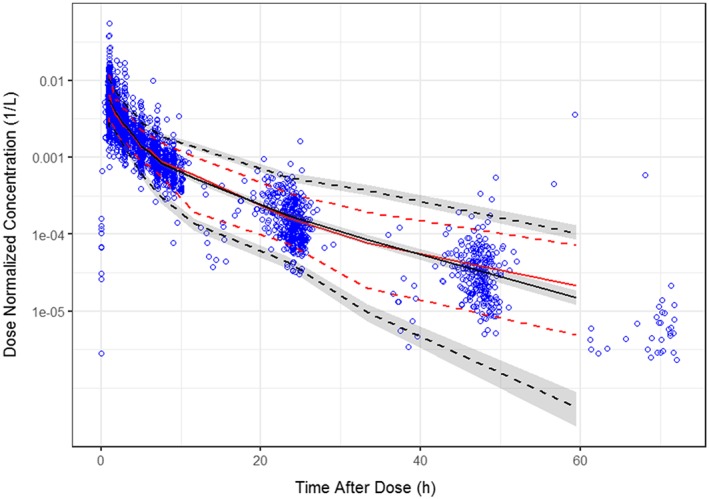
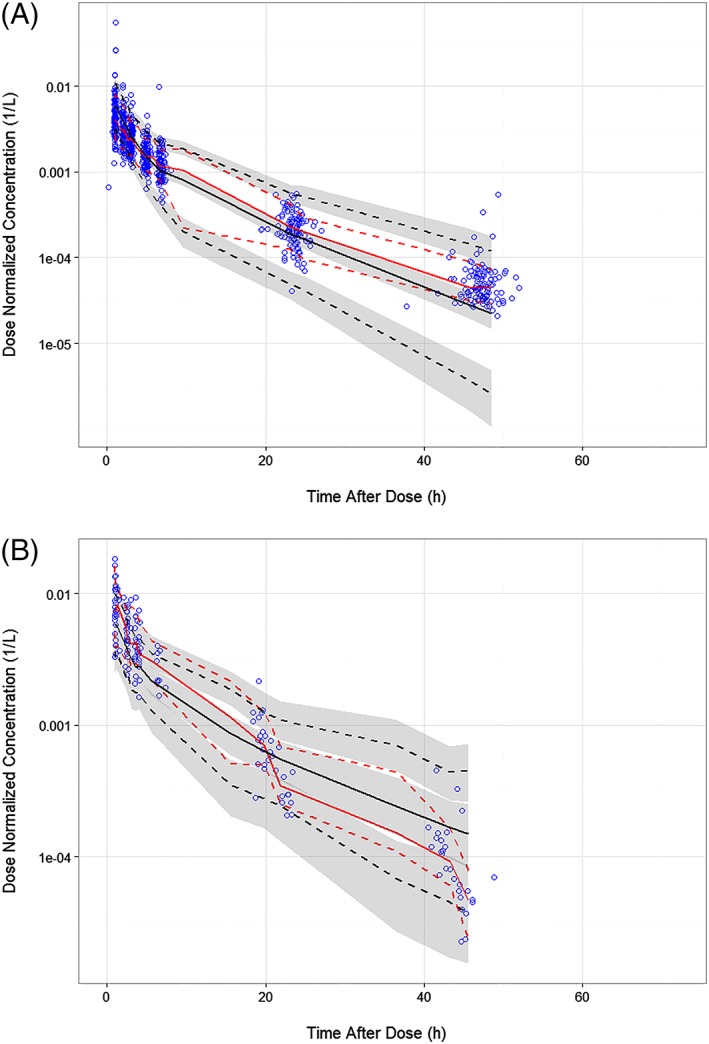
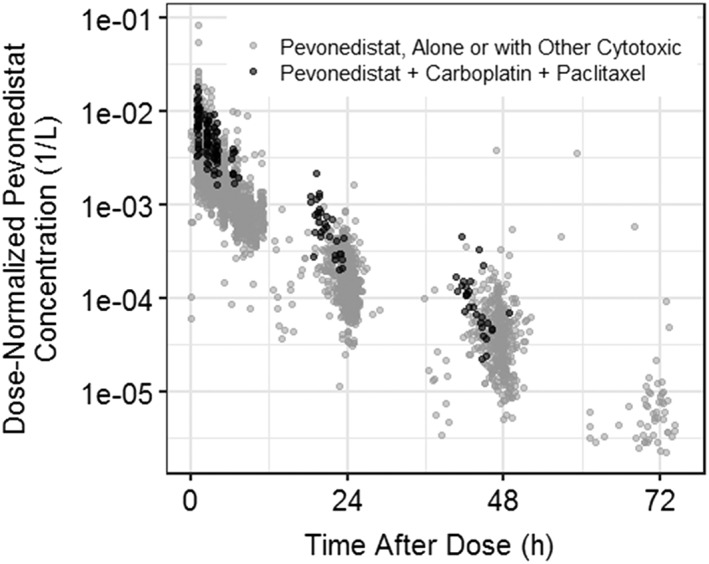
Data were pooled from 6 clinical studies consisting of 335 patients with solid tumours or haematological malignancies administered pevonedistat alone or in combination with azacitidine, docetaxel, carboplatin + paclitaxel, or gemcitabine. Model development and covariate analysis followed standard methods. Parameters and bootstrap 95% confidence intervals were estimated using nonlinear mixed-effects modelling. The final model was evaluated using visual predictive checks and other goodness-of-fit criteria.
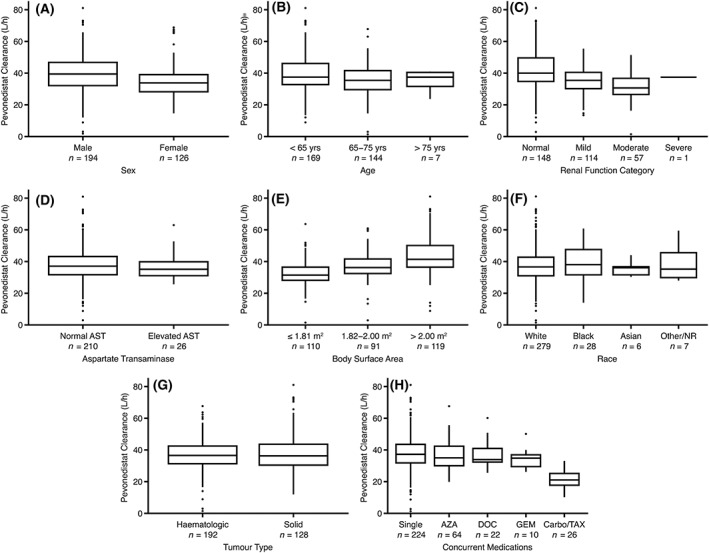
A linear 2-compartment model best described pevonedistat PK. The final model included the effect of body surface area (BSA) on clearance (CL and Q) and volume of distribution of pevonedistat, effect of concomitantly administered carboplatin + paclitaxel on CL, and effect of albumin on Q. Race, sex, age, tumour type (haematological vs solid), mild or moderate renal impairment (creatinine clearance ≥30 mL/min), or mild hepatic impairment, had no impact on pevonedistat PK.
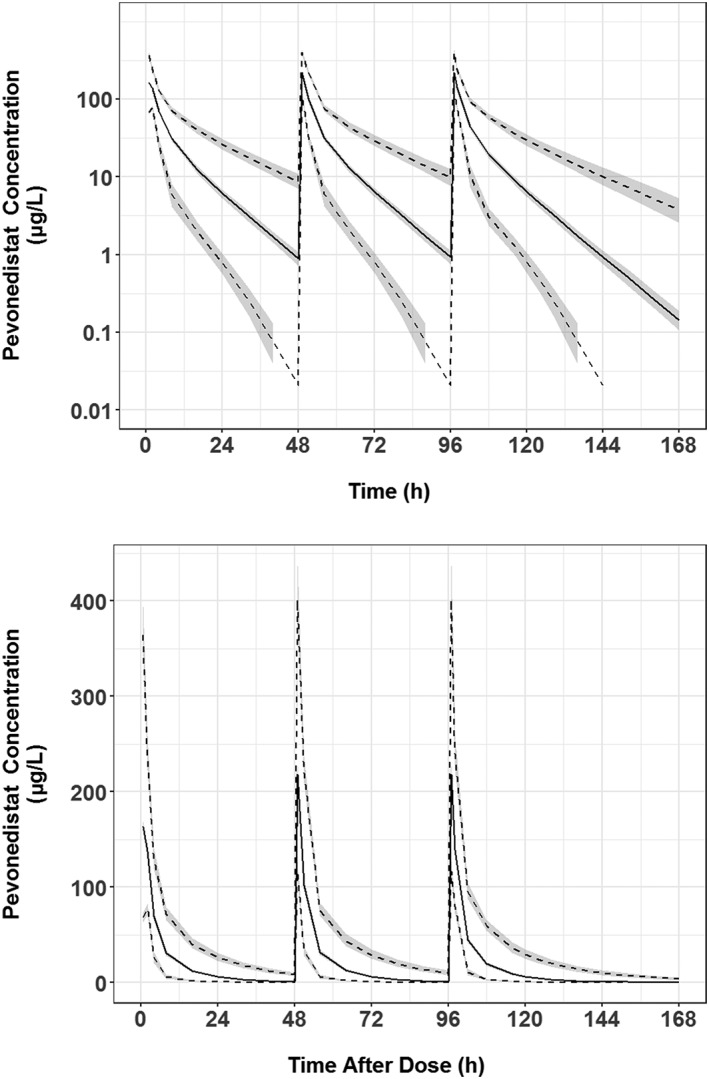
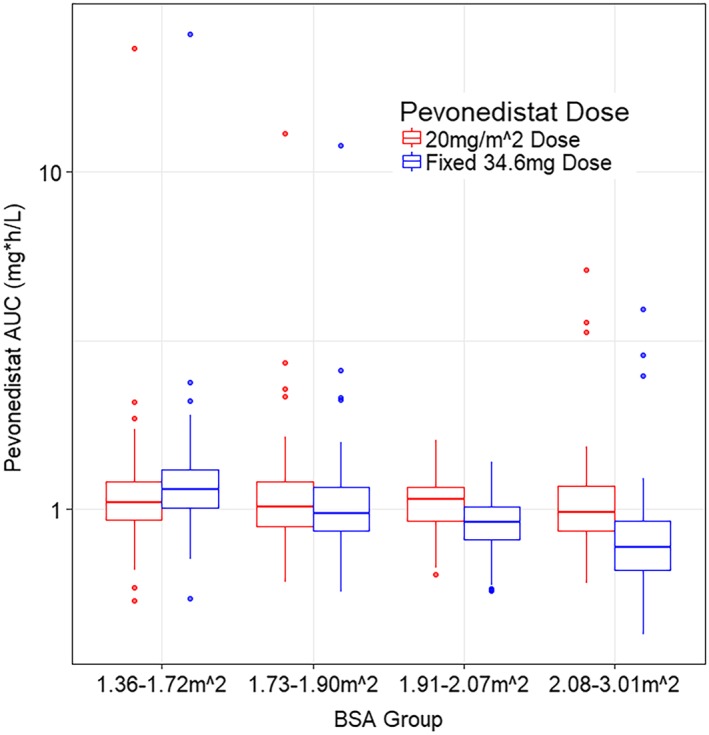
The clinical PK profile of pevonedistat is comparable in patients with solid tumours or haematological malignancies. All PK parameters exhibited ≥20% change over the observed BSA range (1.38-3 m ) with CL ranging from 75.5 to 208% of the reference value, with simulations supporting BSA-based dosing to minimize interindividual variability in drug exposures. Concurrent administration of carboplatin + paclitaxel decreased pevonedistat CL by approximately 44%, while coadministration with azacitidine, gemcitabine or docetaxel did not alter pevonedistat CL. No other factors were identified as influencing pevonedistat PK.
进行群体药代动力学(PK)分析,定量评估患者特征和合并用药因素对培维酮司他 PK 的影响。
汇总了来自 6 项临床研究的数据,这些研究共纳入了 335 例接受培维酮司他单药或联合阿扎胞苷、多西他赛、卡铂+紫杉醇或吉西他滨治疗的实体瘤或血液恶性肿瘤患者。采用标准方法进行模型开发和协变量分析。使用非线性混合效应模型估算参数和自举 95%置信区间。使用可视化预测检查和其他拟合优度标准评估最终模型。
培维酮司他 PK 最佳拟合线性 2 室模型。最终模型纳入了体表面积(BSA)对培维酮司他清除率(CL 和 Q)和分布容积的影响、合并使用卡铂+紫杉醇对 CL 的影响,以及白蛋白对 Q 的影响。种族、性别、年龄、肿瘤类型(血液系统 vs 实体瘤)、轻度或中度肾功能不全(肌酐清除率≥30 mL/min)或轻度肝损伤对培维酮司他 PK 无影响。
在实体瘤或血液恶性肿瘤患者中,培维酮司他的临床 PK 特征相似。所有 PK 参数在观察到的 BSA 范围内(1.38-3 m )变化≥20%,CL 范围为参考值的 75.5%至 208%,模拟结果支持基于 BSA 的剂量方案,以最大限度地减少药物暴露的个体间变异性。卡铂+紫杉醇的合并使用使培维酮司他 CL 降低约 44%,而与阿扎胞苷、吉西他滨或多西他赛合并使用不会改变培维酮司他 CL。未发现其他因素对培维酮司他 PK 有影响。