Maher Keri R, Shafer Danielle, Schaar Dale, Bandyopadhyay Dipankar, Deng Xiaoyan, Wright John, Piekarz Richard, Rudek Michelle A, Harvey R Donald, Grant Steven
Massey Comprehensive Cancer Center, Virginia Commonwealth University, Richmond, VA, USA.
Inova Schar Cancer Center, Fairfax, VA, USA.
Cancer Chemother Pharmacol. 2025 Jan 17;95(1):24. doi: 10.1007/s00280-024-04742-9.
Relapsed and/or refractory acute myeloid leukemia and high-risk myelodysplastic syndrome continue to have a poor prognosis with limited treatment options despite advancements in rational combination and targeted therapies. Belinostat (an HDAC inhibitor) and Pevonedistat (a NEDD8 inhibitor) have each been independently studied in hematologic malignancies and have tolerable safety profiles with limited single-agent activity. Preclinical studies in AML cell lines and primary AML cells show the combination to be highly synergistic, particularly in high-risk phenotypes such as p53 mutant and FLT-3-ITD positive cells. Here, we present the safety, pharmacokinetics and pharmacodynamics of belinostat and pevonedistat in a dose escalation Phase I study in AML and High-Risk MDS.
Eighteen patients (16 with AML, 2 with MDS) were treated at 5 dose levels (belinostat 800-1000 mg/m, pevonedistat 20-50 mg/m). Safety and tolerability were assessed according to protocol defined dose limiting toxicities (DLTs). Correlative pharmacokinetic and pharmacodynamic analyses were performed.
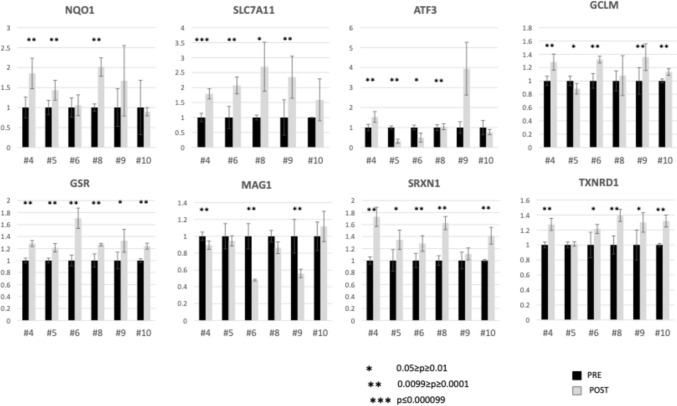
No dose limiting toxicities were noted. Most Grade 3 or 4 toxicities were hematologic in nature. The best response was stable disease in four patients, and complete remission in one patient who qualified as an exceptional responder. Pharmakokinetic studies revealed no association between drug exposure and best response. Pharmacodynamic RT-PCR studies demonstrated post-treatment increases in several proteins, including quantitative increases in the oxidative stress protein NQO1, ferroptosis protein SLC7A11, and GSR, linked to glutathione metabolism and oxidative stress, as did the anti-oxidants SRXN1 and TXNRD1.
Patterns of post-treatment changes in correlative pharmacodynamic parameters may suggest possible mechanistic changes in the DNA damage response, oxidative damage, and ferroptosis pathways. The combination of pevonedistat plus belinosat is safe in an adult relapsed and/or refractory AML/High-Risk MDS population with modest but notable activity in this heavily treated, high risk population. Our findings also raise the possibility that certain extremely poor prognosis AML patients may respond to a regimen combining two targeted agents that have little or no activity when administered individually.
ClinicalTrials.gov ID NCT03772925, first posted 12/12/2018; CTEP Identifier 10246.
复发和/或难治性急性髓系白血病以及高危骨髓增生异常综合征的预后仍然很差,尽管在合理联合治疗和靶向治疗方面取得了进展,但治疗选择仍然有限。贝利司他(一种组蛋白去乙酰化酶抑制剂)和pevonedistat(一种NEDD8抑制剂)各自已在血液系统恶性肿瘤中进行了独立研究,并且具有可耐受的安全性,单药活性有限。在急性髓系白血病细胞系和原发性急性髓系白血病细胞中的临床前研究表明,联合使用具有高度协同作用,特别是在p53突变和FLT-3-ITD阳性细胞等高风险表型中。在此,我们在一项针对急性髓系白血病和高危骨髓增生异常综合征的剂量递增I期研究中展示了贝利司他和pevonedistat的安全性、药代动力学和药效学。
18例患者(16例急性髓系白血病,2例骨髓增生异常综合征)接受了5个剂量水平的治疗(贝利司他800 - 1000mg/m²,pevonedistat 20 - 50mg/m²)。根据方案定义的剂量限制性毒性(DLT)评估安全性和耐受性。进行了相关的药代动力学和药效学分析。
未观察到剂量限制性毒性。大多数3级或4级毒性本质上是血液学毒性。最佳反应是4例患者病情稳定,1例患者完全缓解,该患者被认定为特殊反应者。药代动力学研究表明药物暴露与最佳反应之间无关联。药效学RT-PCR研究显示治疗后几种蛋白质增加,包括氧化应激蛋白NQO1、铁死亡蛋白SLC7A11和与谷胱甘肽代谢及氧化应激相关的GSR定量增加,抗氧化剂SRXN1和TXNRD1也有增加。
相关药效学参数治疗后的变化模式可能提示DNA损伤反应、氧化损伤和铁死亡途径中可能的机制变化。pevonedistat加贝利司他的联合用药在成人复发和/或难治性急性髓系白血病/高危骨髓增生异常综合征患者中是安全的,在这个经过大量治疗的高风险人群中具有适度但显著的活性。我们的研究结果还提出了一种可能性,即某些预后极差的急性髓系白血病患者可能对一种联合两种靶向药物的方案有反应,而这两种药物单独使用时活性很小或没有活性。
ClinicalTrials.gov标识符NCT03772925,首次发布于2018年12月12日;CTEP标识符10246。