Cocoros Noelle M, Ochoa Aileen, Eberhardt Karen, Zambarano Bob, Klompas Michael
Department of Population Medicine, Harvard Medical School and Harvard Pilgrim Health Care Institute, US.
Commonwealth Informatics, US.
EGEMS (Wash DC). 2019 Jul 23;7(1):31. doi: 10.5334/egems.292.
There is scant guidance for defining what denominator to use when estimating disease prevalence via electronic health record (EHR) data.
Describe the intervals between medical encounters to inform the selection of denominators for population-level disease rates, and evaluate the impact of different denominators on the prevalence of chronic conditions.
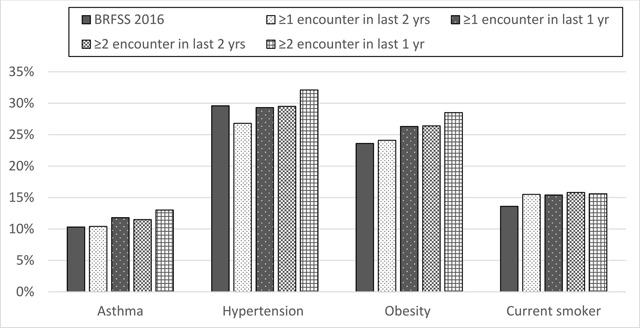
We analyzed the EHRs of three practices in Massachusetts using the Electronic medical record Support for Public Health (ESP) system. We identified adult patients' first medical encounter per year (2011-2016) and counted days to next encounter. We estimated the prevalence of asthma, hypertension, obesity, and smoking using different denominators in 2016: ≥1 encounter in the past one year or two years and ≥2 encounters in the past one year or two years.
In 2011-2016, 1,824,011 patients had 28,181,334 medical encounters. The median interval between encounters was 46, 56, and 66 days, depending on practice. Among patients with one visit in 2014, 82-84 percent had their next encounter within 1 year; 87-91 percent had their next encounter within two years. Increasing the encounter interval from one to two years increased the denominator by 23 percent. The prevalence of asthma, hypertension, and obesity increased with successively stricter denominators - e.g., the prevalence of obesity was 24.1 percent among those with ≥1 encounter in the past two years, 26.3 percent among those with ≥1 encounter in the last one year, and 28.5 percent among those with ≥2 encounters in the past one year.
Prevalence estimates for chronic conditions can vary by >20 percent depending upon denominator. Understanding such differences will inform which denominator definition is best to be used for the need at hand.
在通过电子健康记录(EHR)数据估算疾病患病率时,对于使用何种分母进行定义几乎没有指导意见。
描述医疗就诊之间的间隔时间,为选择人群疾病率的分母提供参考,并评估不同分母对慢性病患病率的影响。
我们使用电子病历公共卫生支持(ESP)系统分析了马萨诸塞州三家医疗机构的电子健康记录。我们确定了成年患者每年(2011 - 2016年)的首次医疗就诊情况,并计算到下一次就诊的天数。我们在2016年使用不同分母估算哮喘、高血压、肥胖和吸烟的患病率:过去一年或两年内≥1次就诊以及过去一年或两年内≥2次就诊。
在2011 - 2016年期间,1,824,011名患者进行了28,181,334次医疗就诊。就诊之间的中位间隔时间为46、56和66天,具体取决于医疗机构。在2014年就诊一次的患者中,82 - 84%在1年内进行了下一次就诊;87 - 91%在两年内进行了下一次就诊。将就诊间隔从一年增加到两年,分母增加了23%。哮喘、高血压和肥胖的患病率随着分母标准越来越严格而增加——例如,肥胖患病率在过去两年内≥1次就诊的人群中为24.1%,在过去一年中≥1次就诊的人群中为26.3%,在过去一年中≥2次就诊的人群中为28.5%。
慢性病患病率的估计值可能因分母不同而相差超过20%。了解这些差异将有助于确定最适合当前需求的分母定义。