Department of Respiratory Medicine, Graduate School of Medicine, Osaka City University, Osaka, Japan.
Internal Medicine III, Wakayama Medical University, Wakayama, Japan.
Cancer Sci. 2019 Oct;110(10):3244-3254. doi: 10.1111/cas.14156. Epub 2019 Aug 30.
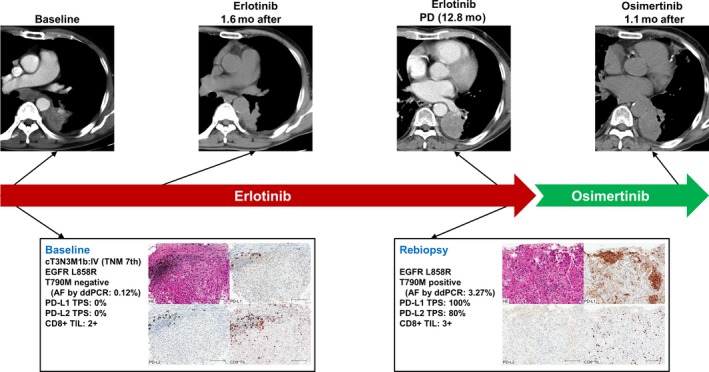
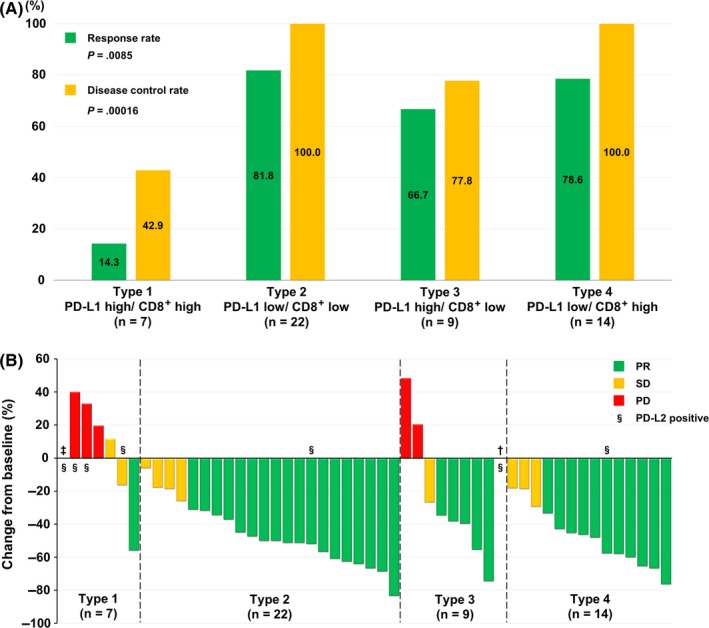
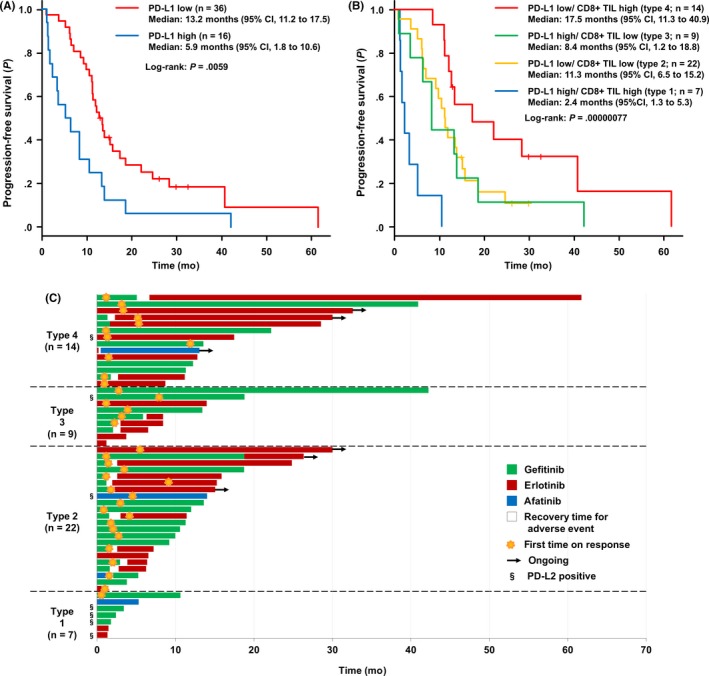
We retrospectively investigated the impact of the tumor microenvironment (TME) on the efficacy of epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) as first-line treatment in 70 patients with advanced EGFR-mutant non-small cell lung cancer and who were seen at Osaka City University Hospital (Osaka, Japan) between August 2013 and December 2017. Using immunohistochemical staining with 28-8 and D7U8C Abs, the tumor proportion score was assessed for programmed cell death-1 ligand-1 (PD-L1), as high (50% or more) or low (less than 50%), and ligand-2 (PD-L2) expression, respectively. The extent of CD8 tumor-infiltrating lymphocytes was evaluated on a scale of 0-3, with 0-1 as low and 2-3 as high. The TME of the 52 evaluable pretreatment specimens was categorized into 4 subtypes, according to the respective PD-L1 tumor proportion and CD8 scores, as follows: (a) high/high (13.5%, n = 7); (b) low/low (42.3%, n = 22); (c) high/low (17.3%, n = 9); and (d) low/high (26.9%, n = 14). Expression of PD-L2 was significantly the highest in type 1 (57.1% vs 4.5% vs 11.1% vs 7.1%, respectively; P = .0090). Response rate was significantly the lowest in type 1 (14.3% vs 81.8% vs 66.7% vs 78.6%, respectively; P = .0085). Progression-free survival was the shortest in type 1 and the longest in type 4 (median, 2.4 vs 11.3 vs 8.4 vs 17.5 months, respectively; P = .00000077). The efficacy of EGFR-TKIs differed according to the TME, and the phenotype with high PD-L1 and CD8 expression might be the subset that would poorly benefit from such treatment.
我们回顾性研究了肿瘤微环境(TME)对 70 例在日本大阪市立大学医院(大阪,日本)就诊的晚期 EGFR 突变非小细胞肺癌患者接受表皮生长因子受体(EGFR)-酪氨酸激酶抑制剂(TKIs)作为一线治疗疗效的影响。使用 28-8 和 D7U8C Abs 的免疫组织化学染色,评估程序性死亡配体-1(PD-L1)和配体-2(PD-L2)的肿瘤比例评分,分别为高(50%或更高)或低(低于 50%)。CD8 肿瘤浸润淋巴细胞的程度根据 0-3 级进行评估,0-1 级为低,2-3 级为高。根据各自的 PD-L1 肿瘤比例和 CD8 评分,将 52 例可评估预处理标本的 TME 分为 4 种亚型:(a)高/高(13.5%,n=7);(b)低/低(42.3%,n=22);(c)高/低(17.3%,n=9);(d)低/高(26.9%,n=14)。PD-L2 的表达在 1 型中显著最高(57.1%比 4.5%比 11.1%比 7.1%,分别;P=0.0090)。反应率在 1 型中最低(14.3%比 81.8%比 66.7%比 78.6%,分别;P=0.0085)。无进展生存期在 1 型中最短,在 4 型中最长(中位数,2.4 比 11.3 比 8.4 比 17.5 个月,分别;P=0.00000077)。EGFR-TKIs 的疗效因 TME 而异,高 PD-L1 和 CD8 表达的表型可能是不太受益于这种治疗的亚组。