Department of Anesthesiology and Critical Care Medicine, The Children's Hospital of Philadelphia, University of Pennsylvania, Philadelphia, PA.
Department of Pediatrics, University of Utah, Salt Lake City, UT.
Crit Care Med. 2019 Nov;47(11):1627-1636. doi: 10.1097/CCM.0000000000003898.
The objective of this study was to associate ventilation rates during in-hospital cardiopulmonary resuscitation with 1) arterial blood pressure during cardiopulmonary resuscitation and 2) survival outcomes.
Prospective, multicenter observational study.
Pediatric and pediatric cardiac ICUs of the Collaborative Pediatric Critical Care Research Network.
Intubated children (≥ 37 wk gestation and < 19 yr old) who received at least 1 minute of cardiopulmonary resuscitation.
None.
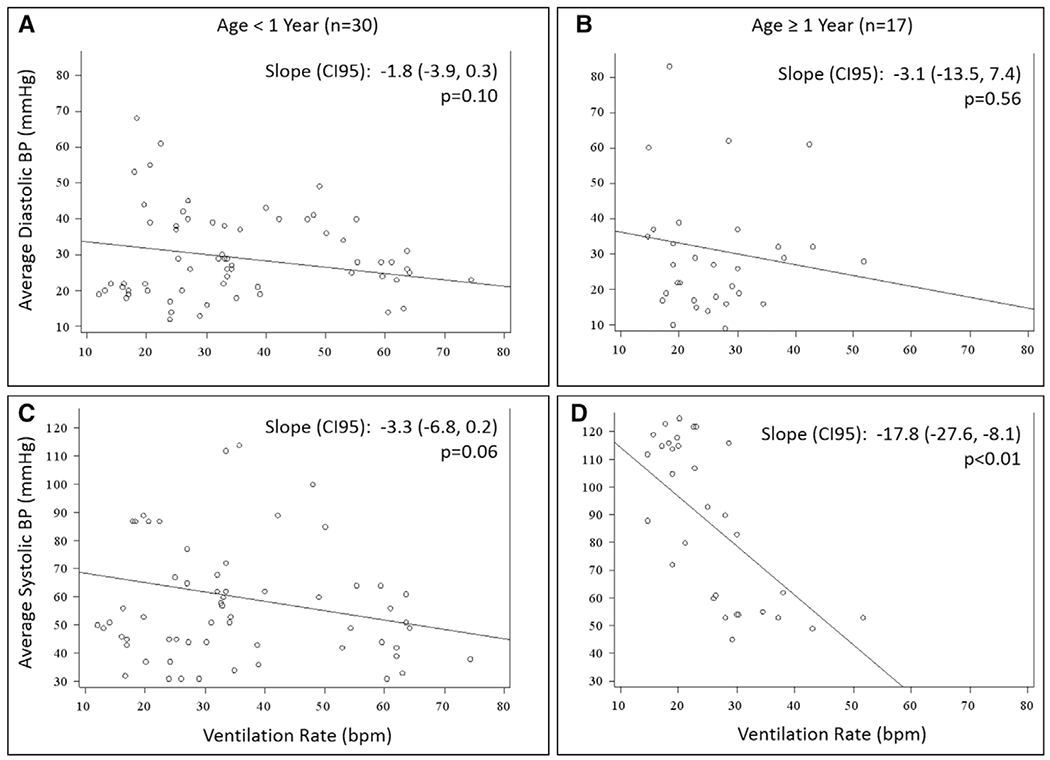
Arterial blood pressure and ventilation rate (breaths/min) were manually extracted from arterial line and capnogram waveforms. Guideline rate was defined as 10 ± 2 breaths/min; high ventilation rate as greater than or equal to 30 breaths/min in children less than 1 year old, and greater than or equal to 25 breaths/min in older children. The primary outcome was survival to hospital discharge. Regression models using Firth penalized likelihood assessed the association between ventilation rates and outcomes. Ventilation rates were available for 52 events (47 patients). More than half of patients (30/47; 64%) were less than 1 year old. Eighteen patients (38%) survived to discharge. Median event-level average ventilation rate was 29.8 breaths/min (interquartile range, 23.8-35.7). No event-level average ventilation rate was within guidelines; 30 events (58%) had high ventilation rates. The only significant association between ventilation rate and arterial blood pressure occurred in children 1 year old or older and was present for systolic blood pressure only (-17.8 mm Hg/10 breaths/min; 95% CI, -27.6 to -8.1; p < 0.01). High ventilation rates were associated with a higher odds of survival to discharge (odds ratio, 4.73; p = 0.029). This association was stable after individually controlling for location (adjusted odds ratio, 5.97; p = 0.022), initial rhythm (adjusted odds ratio, 3.87; p = 0.066), and time of day (adjusted odds ratio, 4.12; p = 0.049).
In this multicenter cohort, ventilation rates exceeding guidelines were common. Among the range of rates delivered, higher rates were associated with improved survival to hospital discharge.
本研究旨在探讨院内心肺复苏期间的通气率与 1)心肺复苏期间的动脉血压和 2)生存结局之间的关联。
前瞻性、多中心观察性研究。
合作儿科危重病研究网络的儿科和儿科心脏 ICU。
接受至少 1 分钟心肺复苏的气管插管患儿(胎龄≥ 37 周且<19 岁)。
无。
从动脉线和二氧化碳描记图波形中手动提取动脉血压和通气率(呼吸/分钟)。指南率定义为 10±2 次/分钟;通气率高定义为<1 岁的儿童大于或等于 30 次/分钟,年龄较大的儿童大于或等于 25 次/分钟。主要结局为出院时存活。使用 Firth 惩罚似然回归模型评估通气率与结局之间的关联。通气率可用于 52 个事件(47 例患者)。超过一半的患者(30/47;64%)年龄小于 1 岁。18 名患者(38%)存活至出院。事件水平平均通气率中位数为 29.8 次/分钟(四分位距,23.8-35.7)。没有事件水平平均通气率符合指南;30 个事件(58%)通气率高。仅在 1 岁或以上的儿童中观察到通气率与动脉血压之间存在显著关联,且仅与收缩压相关(-17.8mmHg/10 次/分钟;95%CI,-27.6 至-8.1;p<0.01)。高通气率与出院时存活的几率更高相关(比值比,4.73;p=0.029)。在分别单独控制位置(调整比值比,5.97;p=0.022)、初始节律(调整比值比,3.87;p=0.066)和时间(调整比值比,4.12;p=0.049)后,该关联仍然稳定。
在这项多中心队列研究中,超过指南的通气率很常见。在所提供的一系列通气率中,较高的通气率与出院时存活率的提高相关。