Translational Health Research Institute (THRI), School of Medicine, Western Sydney University, Campbelltown Campus, Locked Bag 1797, Penrith, NSW, 2571, Australia.
General Practice Unit, Prescot Specialist Medical Centre, Welfare Quarters, Makurdi, Benue State, Nigeria.
BMC Public Health. 2019 Aug 1;19(1):1034. doi: 10.1186/s12889-019-7360-6.
Inappropriate complementary feeding practices significantly contribute to undernutrition among children under 2 years of age in India. However, there is limited up-to-date evidence on the prevalence and factors associated with complementary feeding practices to guide policy actions at the subnational level in India. We investigated the regional prevalence and factors associated with complementary feeding practices in India.
This study used a sample of 69,464 maternal responses from the 2015-16 National Family Health Survey in India. The prevalence of complementary feeding indicators was estimated using data for each administrative region, namely: North (n = 8469), South (n = 12,828), East (n = 18,141), West (n = 8940), North-East (n = 2422) and Central (n = 18,664). Factors associated with complementary feeding by region in India were investigated using logistic regression Generalized Linear Latent and Mixed Models (GLLAMM) with a logit link and binomial family that adjusted for clustering and sampling weights.
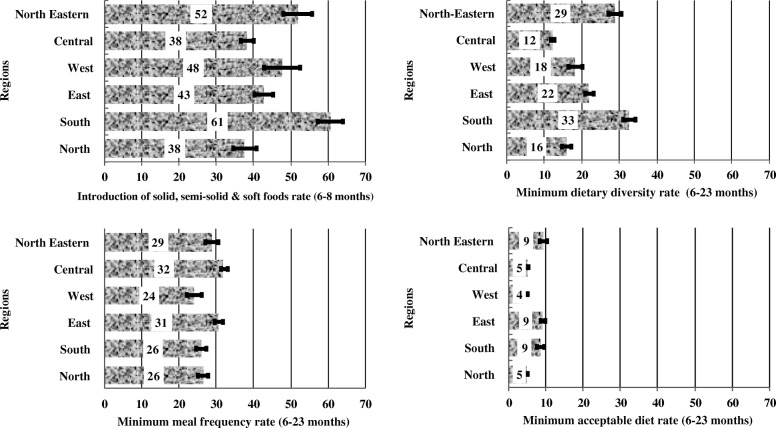
The study showed a wide variation in the prevalence of introduction of solid, semi-solid or soft foods (complementary foods) among infants aged 6-8 months in regional India; highest in the South (61%) and lowest in the Central and Northern regions (38%). Similarly, minimum dietary diversity (MDD) was highest in the South (33%) and lowest in the Central region (12%). Both minimum meal frequency (MMF) and minimum acceptable diet (MAD) varied substantially across the regions. The factors associated with complementary feeding practices also differed across Indian regions. Significant modifiable factors associated with complementary feeding practices included higher household wealth index for the introduction of complementary foods in the North and Eastern India; higher maternal education for MMF and MDD in the North and Central regions; and frequent antenatal care visits (≥4 visits) for all indicators but for different regions.
Our study indicates that there are wide differences in regional prevalence and factors associated with complementary feeding practices in India. The improvement of complementary feeding practices in India would require national and sub-national efforts that target vulnerable mothers, including those with no education and limited health service contacts.
在印度,不合适的补充喂养做法是导致 2 岁以下儿童营养不足的重要原因。然而,目前关于补充喂养做法的流行程度和相关因素的最新证据有限,无法为印度国家以下各级别的政策行动提供指导。我们调查了印度补充喂养做法的地区流行程度和相关因素。
本研究使用了印度 2015-16 年国家家庭健康调查中 69464 名母亲的样本。使用每个行政区域的数据来估计补充喂养指标的流行程度,即:北部(n=8469)、南部(n=12828)、东部(n=18141)、西部(n=8940)、东北部(n=2422)和中部(n=18664)。使用具有对数链接和二项式家族的逻辑回归广义潜在和混合模型(GLLAMM),对印度各地区与补充喂养相关的因素进行调查,同时调整了聚类和抽样权重。
研究表明,印度各地区 6-8 个月婴儿引入固体、半固体或软食(补充食品)的流行程度存在很大差异;南部最高(61%),中部和北部最低(38%)。同样,最低饮食多样性(MDD)在南部最高(33%),在中部最低(12%)。最低用餐频率(MMF)和最低可接受饮食(MAD)在各地区也有很大差异。与补充喂养做法相关的因素也因印度各地区而异。与补充喂养做法相关的显著可改变因素包括北部和东部的家庭财富指数较高,有利于引入补充食品;北部和中部的母亲教育程度较高,有利于 MMF 和 MDD;以及经常进行产前保健(≥4 次),有利于所有指标,但针对不同地区。
我们的研究表明,印度各地区在补充喂养做法的流行程度和相关因素方面存在很大差异。要改善印度的补充喂养做法,需要国家和国家以下各级别的努力,针对弱势母亲,包括那些没有受过教育和接触有限卫生服务的母亲。