Li Lin, Wang Li, Zhai Chun-Juan, Mou Ya-Ru, Wang Jian-Hong, Cui Lian-Qun
Department of Cardiology, Shandong Provincial Hospital affiliated to Shandong University; Jinan-China.
Department of Hematology, Shandong Provincial Hospital affiliated to Shandong University;Jinan-China.
Anatol J Cardiol. 2019 Aug;22(2):68-76. doi: 10.14744/AnatolJCardiol.2019.77009.
It is unknown whether the intravascular ultrasound (IVUS) guidance for percutaneous coronary intervention (PCI) should be routinely used in small-vessel coronary lesions in patients affected by Type 2 diabetes mellitus (T2DM). This study aimed to assess the clinical significance of the IVUS-guided PCI treatment for small-vessel coronary lesions in T2DM.
This was a prospective interventional trial. A total of 228 patients affected by T2DM with stable angina and a positive stress test in the presence of coronary arteriography (CAG) involving small vessels [online measurement reference vessel diameter ≤3.0 mm by means of quantitative coronary angiography (QCA)] were recruited and divided into two groups: an IVUS-guided group (n=120) and a CAG-guided group (n=108). Follow-up PCIs were performed via CAG or IVUS criteria, respectively. Between-group comparisons were made for the number of stents implanted, length, diameter, and high-pressure balloons used post-dilatation. Major adverse cardiac events (MACEs) defined as cardiac death, nonfatal myocardial infarction, and target lesion revascularization (TLR) were the primary endpoint. The value of late lumen loss and proportion of in-stent restenosis (ISR) were the secondary endpoint, all of which were also evaluated during the follow-up period.
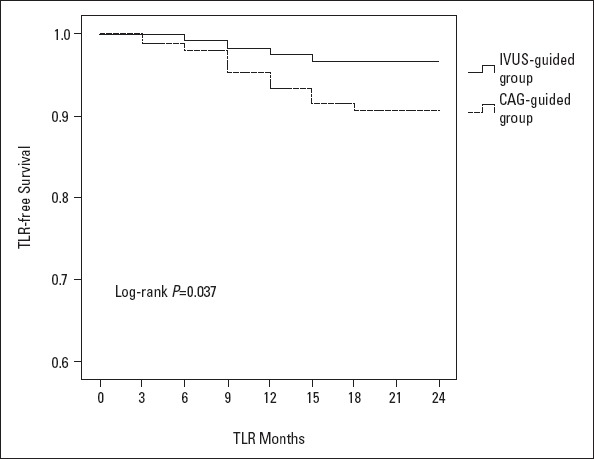
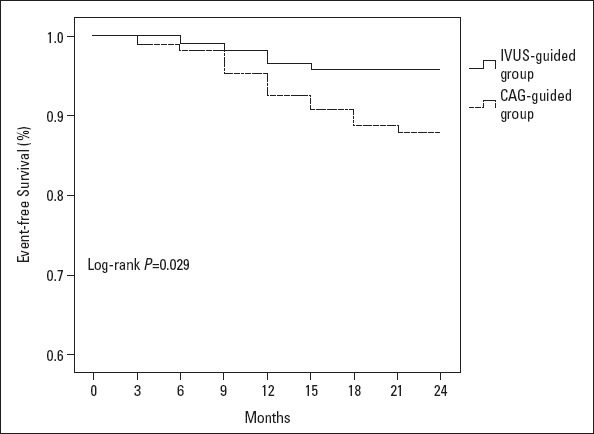
There was an increased lesion length observed using the IVUS measurement when compared with QCA measurements in the IVUS-guided group (p≤0.001). The number of implanted stents, diameter, length, percentage of high-pressure balloons used during post-dilatation, value of late lumen loss, and proportion of ISR decreased in the IVUS-guided group when compared with the CAG-guided group (p=0.002, p=0.001, p=0.003, p=0.004, p=0.007, p=0.001, respectively). After a 2-year follow-up, the Kaplan-Meier curves indicated that the incidence of MACEs was significantly lower in the IVUS-guided group (log-rank p=0.029), mainly because of the TLR reduction (log-rank p=0.037).
The IVUS-guided PCI treatment improved the event-free survival in small-vessel coronary lesions in patients affected by T2DM.
对于2型糖尿病(T2DM)患者的小血管冠状动脉病变,经皮冠状动脉介入治疗(PCI)时血管内超声(IVUS)引导是否应常规使用尚不清楚。本研究旨在评估IVUS引导下PCI治疗T2DM患者小血管冠状动脉病变的临床意义。
这是一项前瞻性干预试验。共纳入228例患有T2DM且有稳定型心绞痛、负荷试验阳性且冠状动脉造影(CAG)显示存在小血管病变[通过定量冠状动脉造影(QCA)在线测量参考血管直径≤3.0 mm]的患者,并将其分为两组:IVUS引导组(n = 120)和CAG引导组(n = 108)。分别根据CAG或IVUS标准进行随访PCI。对两组植入支架的数量、长度、直径以及后扩张时使用的高压球囊进行组间比较。主要不良心脏事件(MACE)定义为心源性死亡、非致命性心肌梗死和靶病变血运重建(TLR),为主要终点。晚期管腔丢失值和支架内再狭窄(ISR)比例为次要终点,所有这些指标在随访期间也进行评估。
与IVUS引导组中QCA测量结果相比,使用IVUS测量观察到病变长度增加(p≤0.001)。与CAG引导组相比,IVUS引导组植入支架的数量、直径、长度、后扩张时使用高压球囊的百分比、晚期管腔丢失值和ISR比例均降低(分别为p = 0.002、p = 0.001、p = 0.003、p = 0.004、p = 0.007、p = 0.001)。经过2年随访,Kaplan-Meier曲线表明IVUS引导组MACE的发生率显著更低(对数秩检验p = 0.029),主要是由于TLR减少(对数秩检验p = 0.037)。
IVUS引导下的PCI治疗改善了T2DM患者小血管冠状动脉病变的无事件生存率。