Department of Neurosurgery, University Hospital Zurich, Frauenklinikstrasse 10, 8091, Zurich, Switzerland.
Clinical Neuroscience Center, University of Zurich, Frauenklinikstrasse 10, 8091, Zurich, Switzerland.
Acta Neurochir (Wien). 2019 Oct;161(10):2073-2082. doi: 10.1007/s00701-019-04021-0. Epub 2019 Aug 3.
Ultrasonic aspiration (UA) devices are commonly used for resecting intracranial tumors, as they allow for internal debulking of large tumors, hereby avoiding damage to adjacent brain tissue during the dissection. Little is known about their comparative safety profiles.
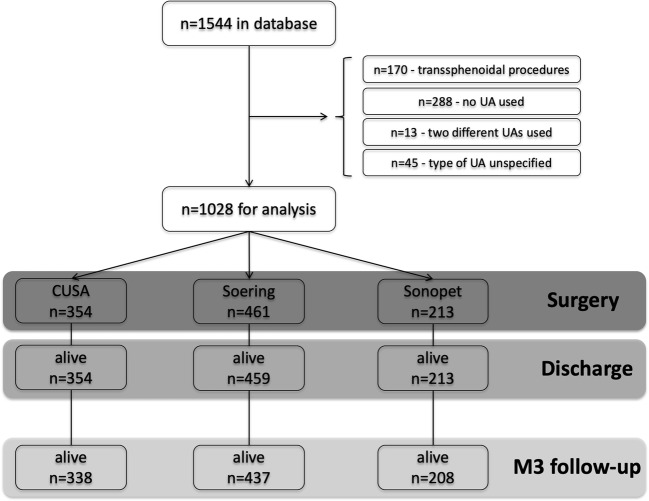
We analyzed data from a prospective patient registry. Procedures using one of the following UA models were included: Integra® CUSA, Söring®, and Stryker® Sonopet. The primary endpoint was morbidity at discharge, defined as significant worsening on the Karnofsky Performance Scale. Secondary endpoints included morbidity and mortality until 3 months postoperative (M3), occurrence, type, and etiology of complications.
Of n = 1028 procedures, the CUSA was used in n = 354 (34.4 %), the Söring in n = 461 (44.8 %), and the Sonopet in n = 213 (20.7 %). There was some heterogeneity of study groups. In multivariable analysis, patients in the Söring (adjusted odds ratio (aOR) 1.29; 95 % confidence interval (CI), 0.80-2.08; p = 0.299), and Sonopet group (aOR, 0.86; 95 % CI, 0.46-1.61; p = 0.645) were as likely as patients in the CUSA group to experience discharge morbidity. At M3, patients in the Söring (aOR, 1.20; 95 % CI, 0.78-1.86; p = 0.415) and Sonopet group (aOR, 0.53; 95 % CI, 0.26-1.08; p = 0.080) were as likely as patients in the CUSA group to experience morbidity. There were also no differences for M3 morbidity in subgroup analyses for gliomas, meningiomas, and metastases. The grade (p = 0.608) and etiology (p = 0.849) of postoperative complications were similar.
Neurosurgeons select UA types with regard to certain case-specific characteristics. The safety profiles of three commonly used UA types appear mostly similar.
超声吸引(UA)装置常用于切除颅内肿瘤,因为它们可以对内部分解大型肿瘤,从而避免在解剖过程中对邻近脑组织造成损伤。关于它们的比较安全性知之甚少。
我们分析了前瞻性患者登记处的数据。包括使用以下 UA 模型之一的程序:Integra® CUSA、Söring® 和 Stryker® Sonopet。主要终点是出院时的发病率,定义为卡诺夫斯基表现量表的显著恶化。次要终点包括术后 3 个月(M3)时的发病率和死亡率、并发症的发生、类型和病因。
在 1028 例手术中,使用 CUSA 354 例(34.4%),Söring 461 例(44.8%),Sonopet 213 例(20.7%)。研究组存在一定的异质性。多变量分析显示,Söring 组(调整后的优势比 (aOR) 1.29;95%置信区间 (CI),0.80-2.08;p=0.299)和 Sonopet 组(aOR,0.86;95%CI,0.46-1.61;p=0.645)的患者与 CUSA 组的患者一样容易出现出院发病率。在 M3 时,Söring 组(aOR,1.20;95%CI,0.78-1.86;p=0.415)和 Sonopet 组(aOR,0.53;95%CI,0.26-1.08;p=0.080)的患者与 CUSA 组的患者一样容易出现发病率。在脑胶质瘤、脑膜瘤和转移瘤的亚组分析中,M3 发病率也没有差异。术后并发症的严重程度(p=0.608)和病因(p=0.849)相似。
神经外科医生根据某些特定的病例特征选择 UA 类型。三种常用的 UA 类型的安全性概况似乎大致相似。