1st Department of Surgery, Semmelweis University, Üllői út 78, Budapest, 1082, Hungary.
Department of Anesthesiology and Intensive Therapy, Semmelweis University, Üllői út 78B, Budapest, 1082, Hungary.
BMC Anesthesiol. 2019 Aug 7;19(1):139. doi: 10.1186/s12871-019-0809-4.
Intraoperative hypotension increases 30-day mortality and the risks of myocardial injury and acute renal failure. Patients with inadequate volume reserve before the induction of anesthesia are highly exposed. The identification of latent hypovolemia is therefore crucial. Ultrasonographic measurement of the inferior vena cava collapsibility index (IVCCI) is able to detect volume responsiveness in circulatory shock. No current evidence is available regarding whether preoperative measurement of the IVCCI could identify patients at high risk for hypotension associated with general anesthesia.
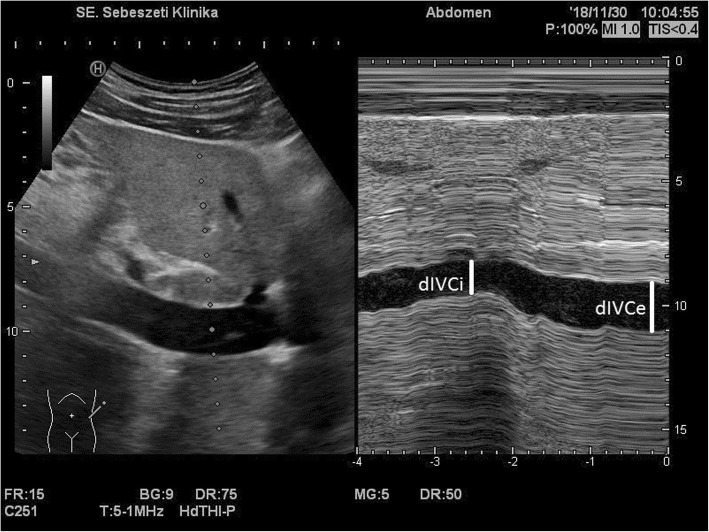
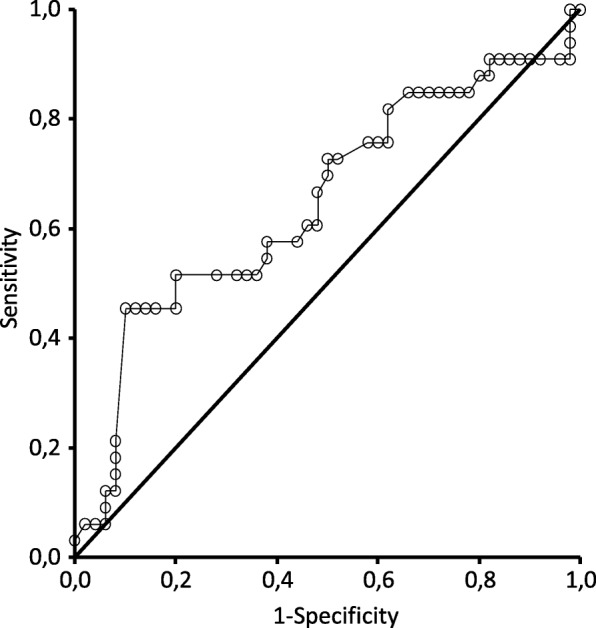
A total of 102 patients undergoing elective general surgery under general anesthesia with standardized propofol induction were recruited for this prospective observational study. The IVCCI was measured under spontaneous breathing. A collapsing (IVCCI≧50%) (CI+) and a noncollapsing (CI-) group were formed. Immediate postinduction changes in systolic and mean blood pressure were compared. The performance of the IVCCI as a diagnostic tool for predicting hypotension (systolic pressure < 90 mmHg or a ≥ 30% drop from the baseline) was evaluated by ROC curve analysis.
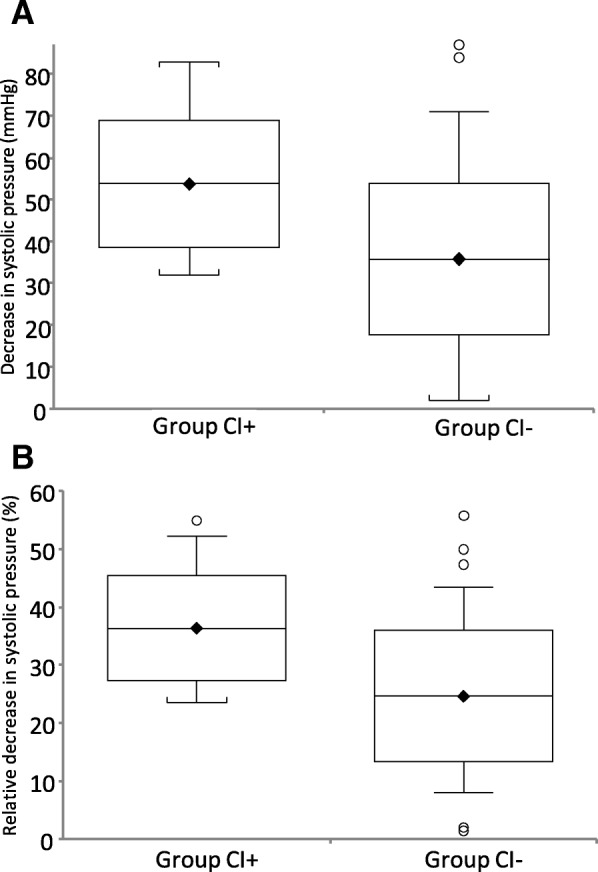
A total of 83 patients were available for analysis, with 20 in the CI+ and 63 in the CI- group, we excluded 19 previously eligible patients due to inadequate visualization of the IVC (7 cases), lack of adherence to the protocol (8 cases), missing data (2 cases) or change in anesthesiologic management (2 cases). The mean decrease in systolic pressure in the CI+ group was 53.8 ± 15.3 compared to 35.8 ± 18.1 mmHg in CI- patients (P = 0.0001). The relative mean arterial pressure change medians were 34.1% (IQR 23.2-43.0%) and 24.2% (IQR 17.2-30.2%), respectively (P = 0.0029). The ROC curve analysis for IVCCI showed an AUC of 64.8% (95% CI 52.1-77.5%). The selected 50% level of the IVCCI had a sensitivity of only 45.5% (95% CI 28.1-63.7%), but the specificity was high at 90.0% (78.2-96.7%). The positive predictive value was 75.0% (95% CI 50.9-91.3%), and the negative predictive value was 71.4% (95% CI 58.7-82.1%).
In spontaneously breathing preoperative noncardiac surgical patients, preoperatively detected IVCCI≧50% can predict postinduction hypotension with high specificity but low sensitivity. Despite moderate performance, IVCCI is an easy, noninvasive and attractive option to identify patients at risk and should be explored further.
术中低血压会增加 30 天死亡率以及心肌损伤和急性肾衰竭的风险。在麻醉诱导前储备容量不足的患者风险极高。因此,识别潜在的血容量不足至关重要。下腔静脉塌陷指数(IVCCI)的超声测量能够检测循环休克中的容量反应性。目前尚无证据表明术前测量 IVCCI 是否可以识别与全身麻醉相关的低血压高危患者。
本前瞻性观察研究共纳入 102 例在全身麻醉下接受择期普外科手术的患者,采用标准化异丙酚诱导。在自主呼吸下测量 IVCCI。形成下腔静脉塌陷(IVCCI≧50%)(CI+)和不下腔静脉塌陷(CI-)组。比较诱导后即刻收缩压和平均血压的变化。通过 ROC 曲线分析评估 IVCCI 作为预测低血压(收缩压<90mmHg 或基线下降≥30%)的诊断工具的性能。
共有 83 例患者可进行分析,其中 CI+组 20 例,CI-组 63 例,我们排除了 19 例之前符合条件的患者,原因是 IVC 显示不佳(7 例)、不符合方案(8 例)、数据缺失(2 例)或麻醉管理改变(2 例)。CI+组收缩压平均下降 53.8±15.3mmHg,而 CI-组为 35.8±18.1mmHg(P=0.0001)。平均动脉压变化中位数分别为 34.1%(IQR 23.2-43.0%)和 24.2%(IQR 17.2-30.2%)(P=0.0029)。IVCCI 的 ROC 曲线分析显示 AUC 为 64.8%(95%CI 52.1-77.5%)。IVCCI 选择的 50%水平的敏感性仅为 45.5%(95%CI 28.1-63.7%),但特异性很高,为 90.0%(78.2-96.7%)。阳性预测值为 75.0%(95%CI 50.9-91.3%),阴性预测值为 71.4%(95%CI 58.7-82.1%)。
在自主呼吸的术前非心脏手术患者中,术前检测到的 IVCCI≧50%可以预测诱导后低血压,具有较高的特异性但较低的敏感性。尽管表现中等,但 IVCCI 是一种简单、无创且有吸引力的选择,可以识别高危患者,应进一步探讨。