Abellán-Galiana Pablo, Fajardo-Montañana Carmen, Riesgo-Suárez Pedro, Pérez-Bermejo Marcelino, Ríos-Pérez Celia, Gómez-Vela José
Department of Endocrinology, Hospital General Universitari de Castelló, Castellón, Spain.
Department of Medicine, Universidad Cardenal Herrera-CEU, CEU Universities, Castellón, Spain.
Endocr Connect. 2019 Sep;8(9):1262-1272. doi: 10.1530/EC-19-0297.
To analyze the usefulness of plasma ACTH in predicting CD remission after surgery and to evaluate the prognostic usefulness of ACTH measurement after the cortisol and ACTH nadir (48 h prior to discharge).
A prospective study was made of 65 patients with CD operated upon between 2005 and 2016.
Postsurgery plasma ACTH and cortisol were measured every 6 h, in the absence of corticosteroid coverage. Hydrocortisone was started in the presence of adrenal insufficiency or cortisol <55.2 nmol/L. Plasma ACTH was again determined before discharge.
Usefulness of plasma ACTH in predicting CD remission.
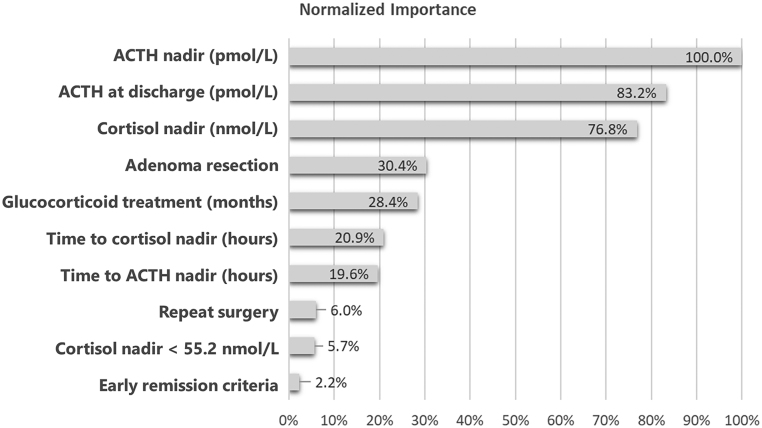
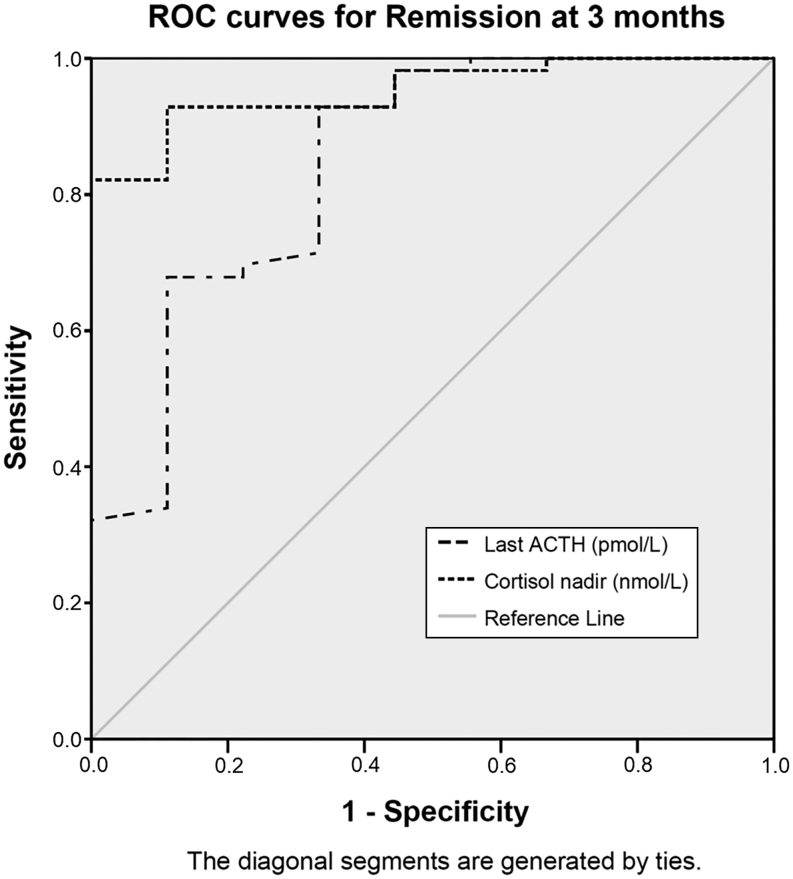
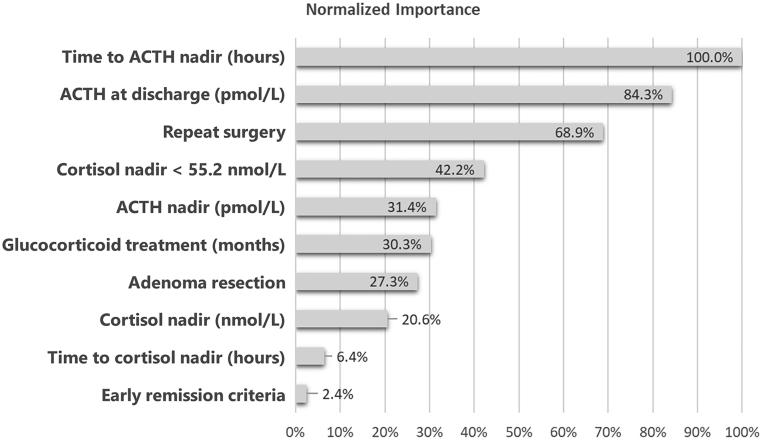
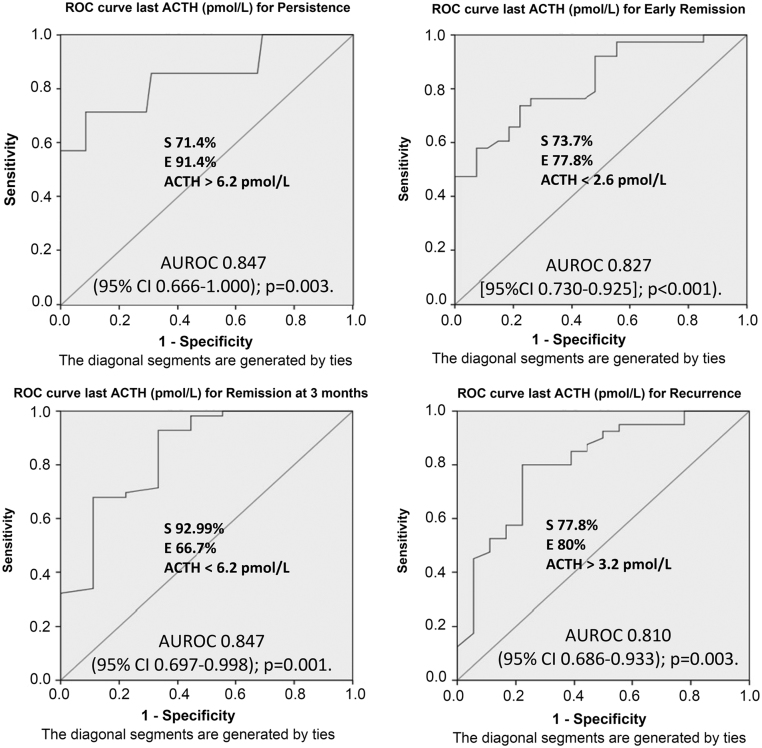
Remission at 3 months of CD was achieved in 56 of 65 cases, with late recurrence in 18 of 58 cases. Following resection, the ACTH nadir was significantly lower referred to late remission (2.8 vs 6.5 pmol/L; P = 0.031) and higher for recurrence (2.1 vs 4.8 pmol/L; P < 0.001), and identical results were obtained for the ACTH values before discharge. In the analysis of the ROC curves, nadir and before discharge ACTH values <1.9 pmol/L and <2.6 pmol/L were respectively indicative of early remission (AUC 0.827; P < 0.001); <6.2 pmol/L of remission at 3 months (AUC 0.847; P = 0.001) and >3.2 pmol/L of recurrence (AUC 0.810; P < 0.001) in both ACTH values. A time to ACTH nadir <46 h was indicative of early remission (AUC 0.751; P = 0.001), while a time >39 h was indicative of recurrence (AUC 0.773; P = 0.001).
We propose an ACTH value <3.3 pmol/L as a good long-term prognostic marker in the postoperative period of CD. Reaching the ACTH nadir in less time is associated to a lesser recurrence rate.
分析血浆促肾上腺皮质激素(ACTH)在预测克罗恩病(CD)术后缓解中的作用,并评估在皮质醇和ACTH最低点(出院前48小时)后测量ACTH的预后价值。
对2005年至2016年间接受手术的65例CD患者进行了一项前瞻性研究。
在无皮质类固醇覆盖的情况下,每6小时测量一次术后血浆ACTH和皮质醇。在出现肾上腺功能不全或皮质醇<55.2 nmol/L时开始使用氢化可的松。出院前再次测定血浆ACTH。
血浆ACTH在预测CD缓解中的作用。
65例患者中有56例在3个月时达到CD缓解,58例中有18例出现晚期复发。切除术后,ACTH最低点明显低于晚期缓解者(2.8对6.5 pmol/L;P = 0.031),高于复发者(2.1对4.8 pmol/L;P < 0.001),出院前ACTH值也得到相同结果。在ROC曲线分析中,最低点和出院前ACTH值<1.9 pmol/L和<2.6 pmol/L分别提示早期缓解(AUC 0.827;P < 0.001);ACTH值<6.2 pmol/L提示3个月时缓解(AUC 0.847;P = 0.001),>3.2 pmol/L提示复发(AUC 0.810;P < 0.001)。ACTH最低点出现时间<46小时提示早期缓解(AUC 0.751;P = 0.001),而>39小时提示复发(AUC 0.773;P = 0.001)。
我们提出ACTH值<3.3 pmol/L作为CD术后良好的长期预后标志物。在更短时间内达到ACTH最低点与较低的复发率相关。