Mays Cancer Center UT Health San Antonio, San Antonio, TX.
Fox Chase Cancer Center, Philadelphia, PA.
Urol Oncol. 2019 Oct;37(10):688-695. doi: 10.1016/j.urolonc.2019.05.017. Epub 2019 Aug 6.
Prostate cancer is the second leading cause of cancer death in men in the US. Since 2015, landmark studies have demonstrated improved survival outcomes with the use of docetaxel (DCT) or abiraterone (AA) in addition to androgen deprivation therapy (ADT) in the metastatic hormone-naïve setting. These treatment strategies have not been prospectively compared but have similar overall survival benefits despite differing mechanisms of action, toxicity, and cost. We performed a cost-effectiveness analysis to provide insight into the value of AA vs. DCT in the first-line treatment of metastatic prostate cancer.
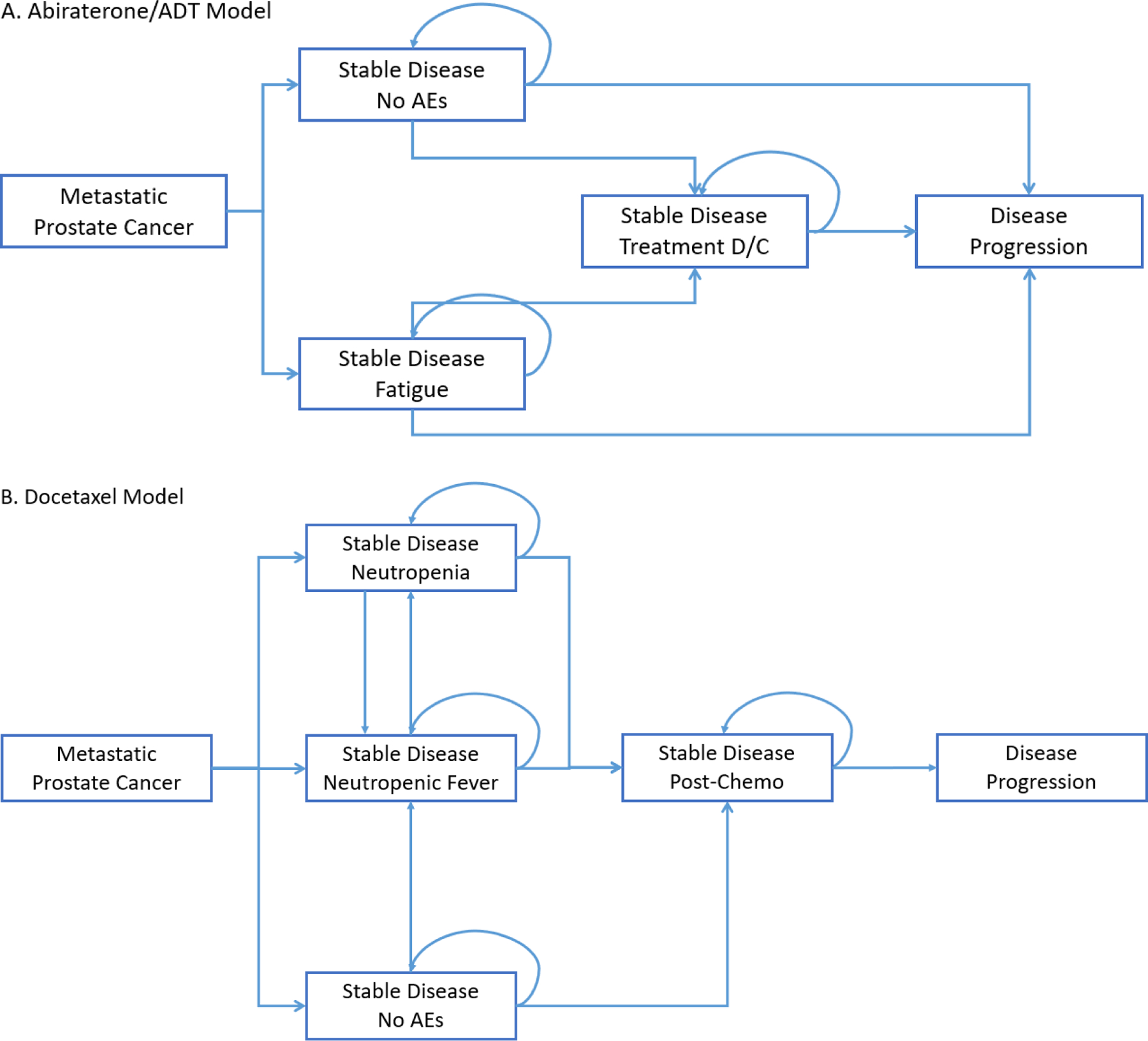
We developed Markov models by using a US-payer perspective and a 3-year time horizon to estimate costs (2018 US$) and progression-free quality-adjusted life years (PF-QALYs) for ADT alone, DCT, and AA. Health states were defined as initial state, treatment states according to experience of an adverse event, and progressed disease/death. State transition probabilities were derived from rates for drug discontinuation, frequency of adverse events, disease progression, and death from the randomized phase III trials ChemoHormonal Therapy Versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer (CHAARTED) and LATITUDE. Univariate and probabilistic sensitivity analyses were conducted to evaluate model uncertainty.
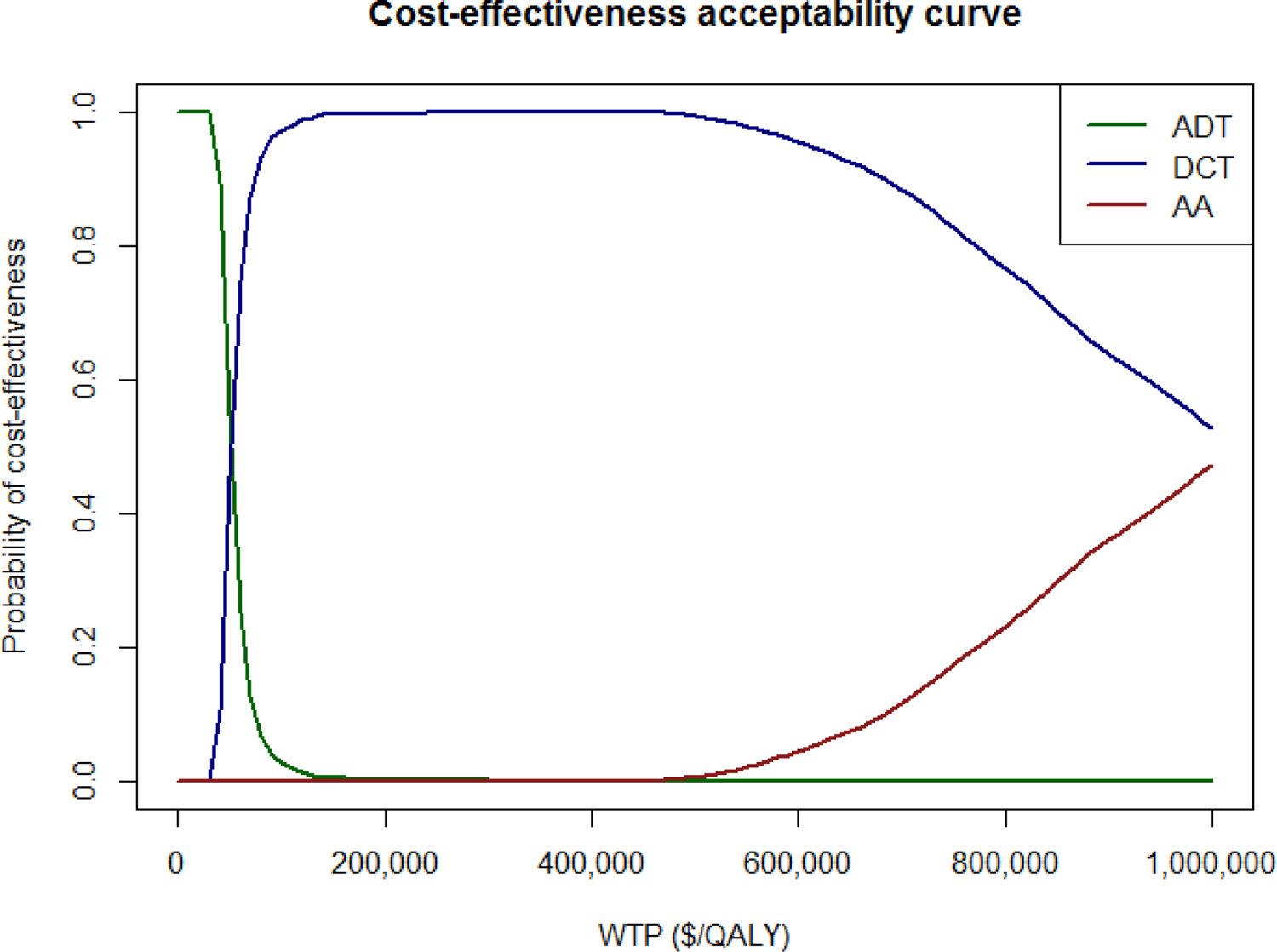
DCT resulted in an increase of 0.32 PF-QALYs and $16,100 in cost and AA resulted in an increase of 0.52 PF-QALYs and $215,800 in cost compared to ADT alone. The incremental cost-effectiveness ratio for DCT vs. ADT was $50,500/PF-QALY and for AA vs. DCT was $1,010,000/PF-QALY. Probabilistic sensitivity analysis demonstrated that at a willingness-to-pay threshold of $150,000/PF-QALY AA was highly unlikely to be cost-effective.
DCT is substantially more cost-effective than AA in the treatment of metastatic hormone naïve prostate cancer.
前列腺癌是美国男性癌症死亡的第二大主要原因。自 2015 年以来,具有里程碑意义的研究表明,在转移性去势敏感环境中,除雄激素剥夺治疗(ADT)外,使用多西他赛(DCT)或阿比特龙(AA)可改善生存结果。这些治疗策略并未进行前瞻性比较,但具有相似的总生存获益,尽管作用机制、毒性和成本不同。我们进行了成本效益分析,以深入了解 AA 与 DCT 在转移性前列腺癌一线治疗中的价值。
我们使用美国支付者的观点和 3 年时间范围,通过开发 Markov 模型,估计 ADT 单药、DCT 和 AA 的成本(2018 年的美元)和无进展质量调整生命年(PF-QALYs)。健康状态定义为初始状态、根据不良事件发生经验的治疗状态以及进展疾病/死亡状态。状态转移概率来自随机 III 期试验 ChemoHormonal Therapy Versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer(CHAARTED)和 LATITUDE 中药物停药、不良事件发生频率、疾病进展和死亡的速率。进行了单变量和概率敏感性分析以评估模型不确定性。
与 ADT 单药相比,DCT 增加了 0.32 个 PF-QALYs 和 16100 美元的成本,而 AA 增加了 0.52 个 PF-QALYs 和 215800 美元的成本。DCT 与 ADT 相比的增量成本效益比为 50500 美元/PF-QALY,AA 与 DCT 相比的增量成本效益比为 1010000 美元/PF-QALY。概率敏感性分析表明,在愿意支付 150000 美元/PF-QALY 的阈值下,AA 极不可能具有成本效益。
在治疗转移性去势敏感前列腺癌方面,DCT 明显比 AA 更具成本效益。