Interdisciplinary Stem Cell Institute, Leonard M Miller School of Medicine, University of Miami, USA.
Hospital Israelita Albert Einstein, São Paulo, Brazil.
Cell Transplant. 2019 Nov;28(11):1390-1403. doi: 10.1177/0963689719860826. Epub 2019 Aug 13.
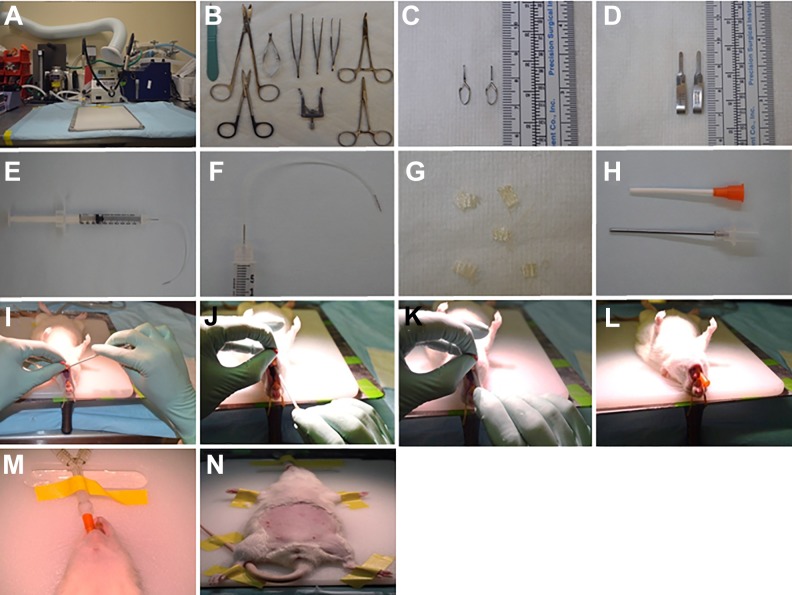
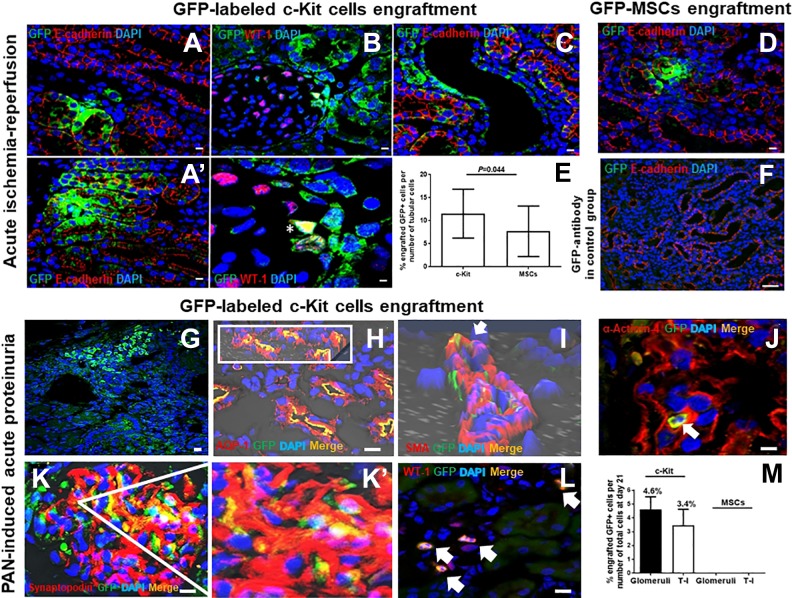
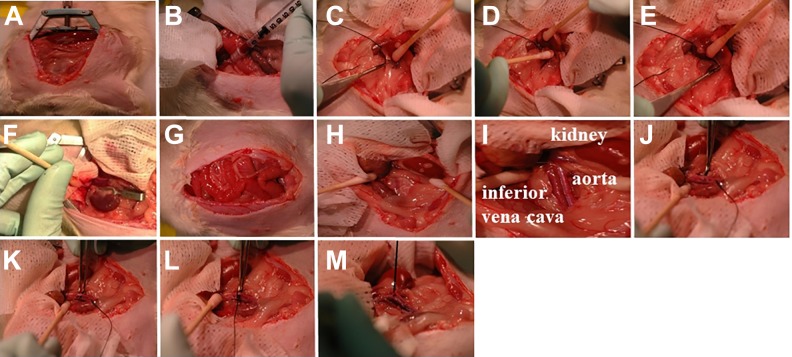
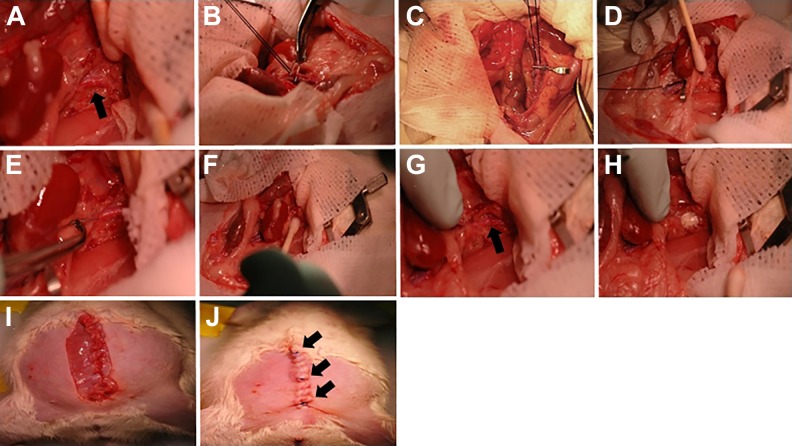
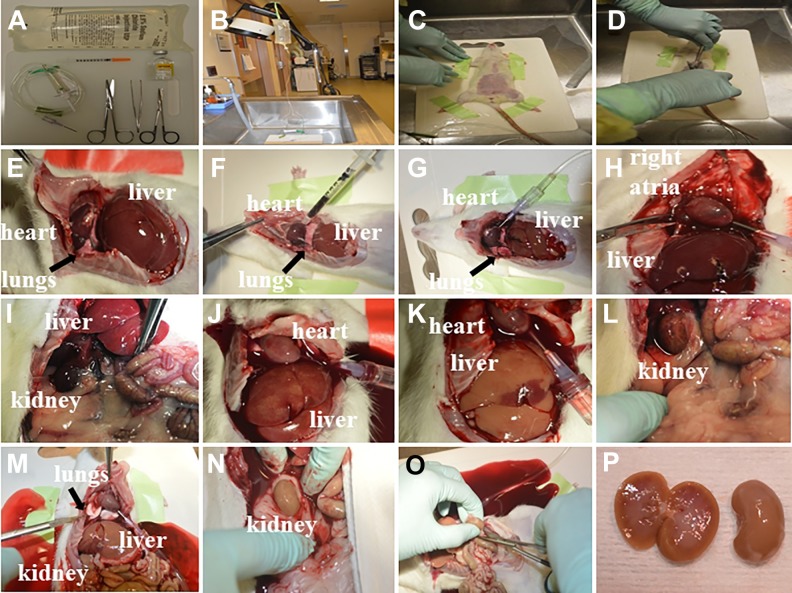
Progenitor/stem cell-based kidney regenerative strategies are a key step towards the development of novel therapeutic regimens for kidney disease treatment. However, the route of cell delivery, e.g., intravenous, intra-arterial, or intra-parenchymal, may affect the efficiency for kidney repair in different models of acute and chronic injury. Here, we describe a protocol of intra-aorta progenitor/stem cell injection in rats following either acute ischemia-reperfusion injury or acute proteinuria induced by puromycin aminonucleoside (PAN) - the experimental prototype of human minimal change disease and early stages of focal and segmental glomerulosclerosis. Vascular clips were applied across both renal pedicles for 35 min, or a single dose of PAN was injected via intra-peritoneal route, respectively. Subsequently, 2 x 10 stem cells [green fluorescent protein (GFP)-labeled c-Kit+ progenitor/stem cells or GFP-mesenchymal stem cells] or saline were injected into the suprarenal aorta, above the renal arteries, after application of a vascular clip to the abdominal aorta below the renal arteries. This approach contributed to engraftment rates of ∼10% at day 8 post ischemia-reperfusion injury, when c-Kit+ progenitor/stem cells were injected, which accelerated kidney recovery. Similar rates of engraftment were found after PAN-induced podocyte damage at day 21. With practice and gentle surgical technique, 100% of the rats could be injected successfully, and, in the week following injection, ∼ 85% of the injected rats will recover completely. Given the similarities in mammals, much of the data obtained from intra-arterial delivery of progenitor/stem cells in rodents can be tested in translational research and clinical trials with endovascular catheters in humans.
基于祖细胞/干细胞的肾脏再生策略是开发肾脏疾病治疗新治疗方案的关键步骤。然而,细胞输送途径,例如静脉内、动脉内或肾实质内,可能会影响不同急性和慢性损伤模型中肾脏修复的效率。在这里,我们描述了在急性缺血再灌注损伤或嘌呤霉素氨基核苷(PAN)诱导的急性蛋白尿后,通过腹主动脉内注射祖细胞/干细胞在大鼠中的方案 - PAN 是人类微小病变病和局灶性和节段性肾小球硬化的早期阶段的实验原型。分别用血管夹夹住双侧肾蒂 35 分钟,或单次腹腔内注射 PAN。随后,在应用血管夹夹住肾动脉下方的腹主动脉后,将 2 x 10 个干细胞[绿色荧光蛋白(GFP)标记的 c-Kit+祖细胞/干细胞或 GFP 间充质干细胞]或生理盐水注入肾上主动脉,位于肾动脉上方。当注射 c-Kit+祖细胞/干细胞时,这种方法有助于在缺血再灌注损伤后 8 天达到约 10%的植入率,从而加速肾脏恢复。在 PAN 诱导的足细胞损伤后 21 天也发现了类似的植入率。通过实践和温和的手术技术,可以成功地对 100%的大鼠进行注射,并且在注射后的一周内,约 85%的注射大鼠将完全恢复。鉴于哺乳动物之间的相似性,可以在人类中使用血管内导管进行转化研究和临床试验,测试在啮齿动物中经动脉内递送祖细胞/干细胞获得的大部分数据。