Peng Yufu, Liu Fei, Xu Hongwei, Lan Xiang, Wei Yonggang, Li Bo
Department of Liver Surgery, Center of Liver Transplantation, West China Hospital of Sichuan University, Chengdu, China.
J Laparoendosc Adv Surg Tech A. 2019 Sep;29(9):1144-1151. doi: 10.1089/lap.2019.0362. Epub 2019 Aug 14.
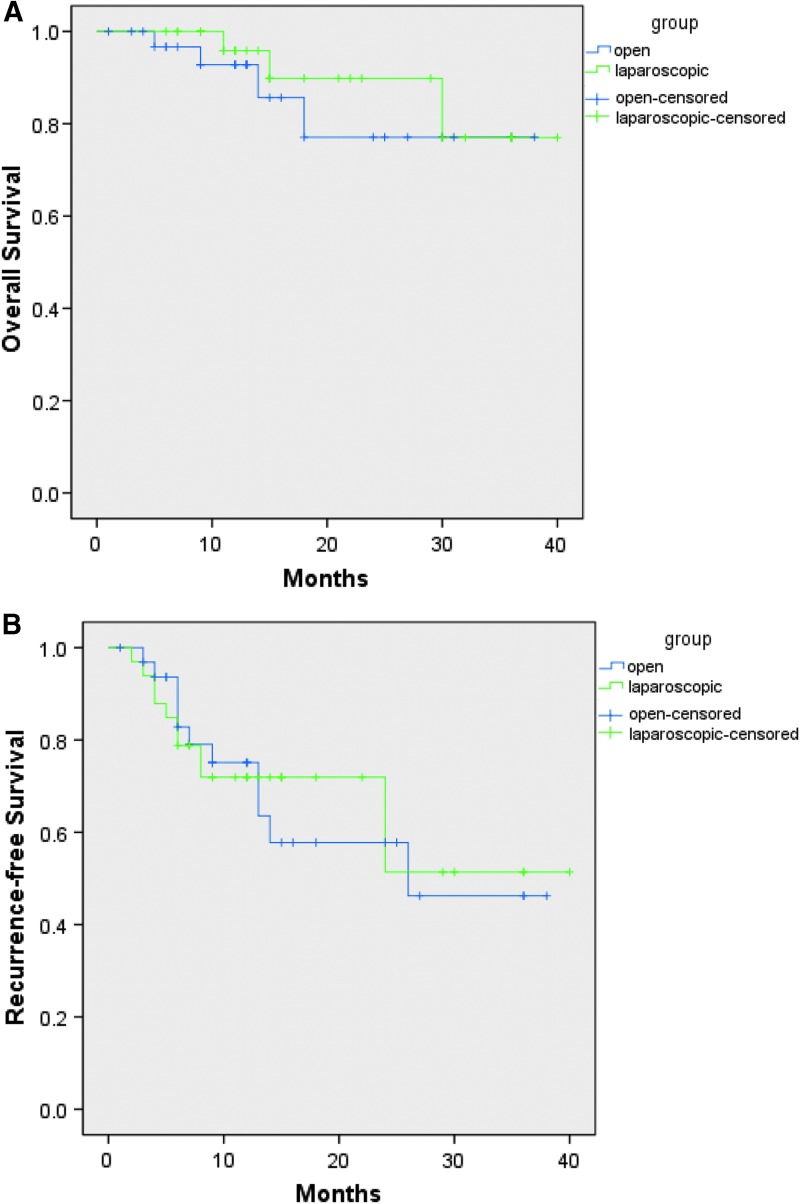
Until now, there is little knowledge about the value of laparoscopic liver resection (LLR) for patients with multiple hepatocellular carcinomas (HCC). This study was performed to assess the efficacy and outcomes of LLR versus open liver resection (OLR) for patients with multiple HCC meeting the Milan criteria. One hundred fifteen patients with multiple HCC meeting the Milan criteria who underwent liver resection from April 2015 to March 2018 were enrolled into this study. According to the different surgical procedures, patients were divided into LLR group and OLR group. Perioperative and oncological outcomes were compared between the two groups after propensity score matching (PSM) with 1:1 match. Thirty three patients were included into each group after PSM with well-balanced basic level. The intraoperative blood loss in LLR group was less than OLR group before PSM (median, 200 vs. 300 mL, = .004), but the difference was not statistically significant after PSM (median, 200 vs. 300 mL, = .064). LLR group showed shorter postoperative hospital stay when compared with OLR group (median, 7 vs. 8 days, respectively, = .014). The perioperative complications and early mortality were comparable in both groups. There were no significant differences in the term of overall survival (OS. = .502) or recurrence-free survival (RFS. = .887) between the two groups after PSM. LLR could be safely and feasibly performed for patients with multiple HCC meeting the Milan criteria in selected patients. It does not increase the risks of postoperative complications and has a similar oncological outcomes compared to OLR.
到目前为止,对于多发性肝细胞癌(HCC)患者行腹腔镜肝切除术(LLR)的价值了解甚少。本研究旨在评估符合米兰标准的多发性HCC患者行LLR与开腹肝切除术(OLR)的疗效和结果。纳入2015年4月至2018年3月期间接受肝切除术的115例符合米兰标准的多发性HCC患者。根据不同的手术方式,将患者分为LLR组和OLR组。在进行1:1倾向评分匹配(PSM)后,比较两组的围手术期和肿瘤学结果。PSM后,每组纳入33例患者,基本水平均衡。PSM前,LLR组术中失血量少于OLR组(中位数分别为200 vs. 300 mL,P = .004),但PSM后差异无统计学意义(中位数分别为200 vs. 300 mL,P = .064)。与OLR组相比,LLR组术后住院时间更短(中位数分别为7天和8天,P = .014)。两组围手术期并发症和早期死亡率相当。PSM后,两组在总生存期(OS,P = .502)或无复发生存期(RFS,P = .887)方面无显著差异。对于符合米兰标准的多发性HCC患者,在选定患者中可以安全、可行地进行LLR。与OLR相比,它不会增加术后并发症的风险,并且具有相似的肿瘤学结果。