Nutrition and Clinical Services Division, International Centre For Diarrhoeal Disease Research, Bangladesh (icddr,b), 63 Shaheed Taj Uddin Ahmed Sarani, Mohakhali, Dhaka, Bangladesh.
PATH, Dr. Gopal Das Bhawan, New Delhi, India.
PLoS Negl Trop Dis. 2019 Aug 15;13(8):e0007653. doi: 10.1371/journal.pntd.0007653. eCollection 2019 Aug.
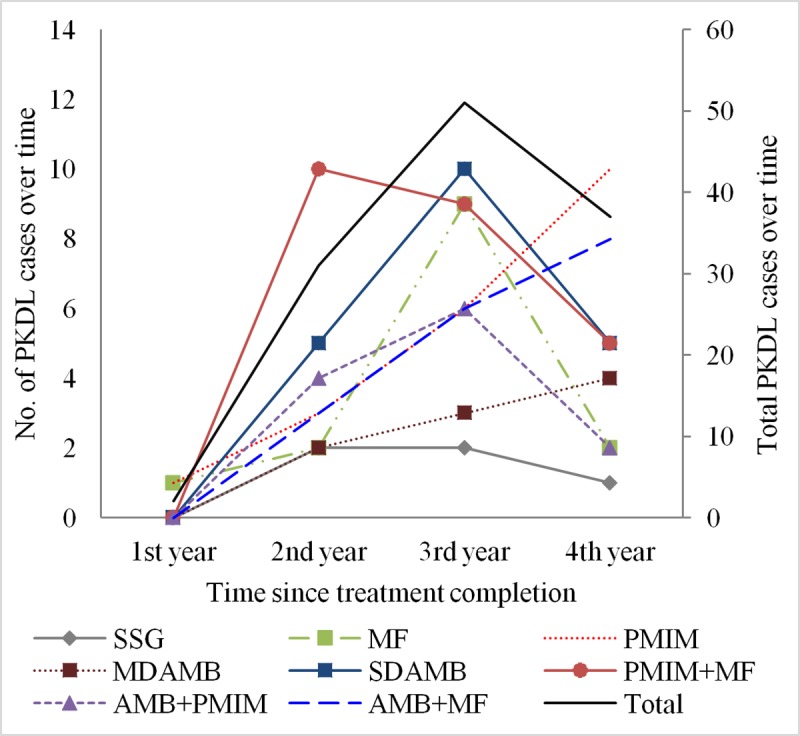
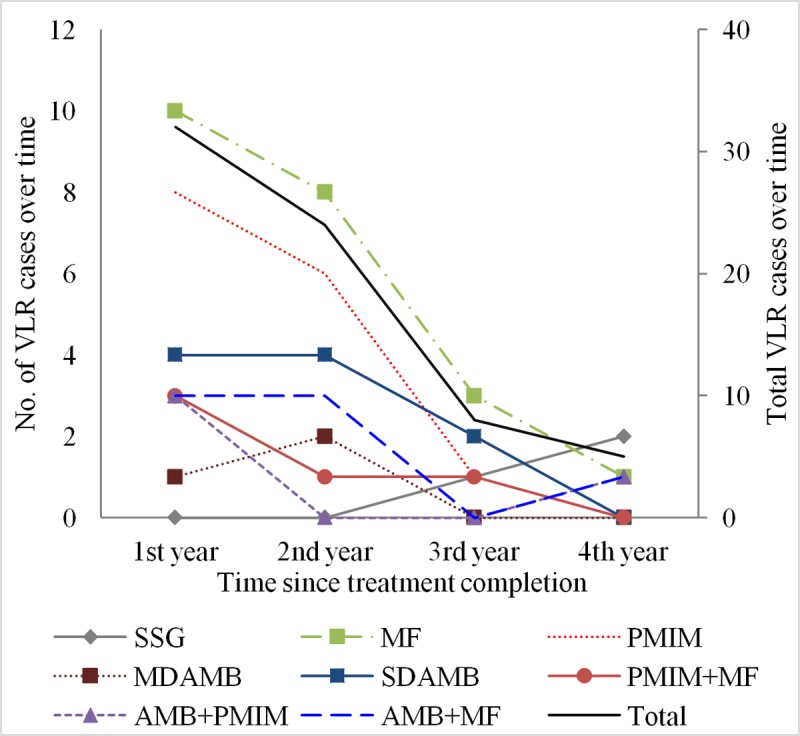
We investigated the relationship of treatment regimens for visceral leishmaniasis (VL) with post-kala-azar dermal leishmaniasis (PKDL) and visceral leishmaniasis relapse (VLR) development.
Study subjects included cohorts of patients cured of VL since treatment with monotherapy by sodium stibogluconate (SSG), miltefosine (MF), paromomycin intramuscular injection (PMIM), liposomal amphotericin B [AmBisome (AMB)] in a single dose (SDAMB) and in multidose (MDAMB), and combination therapies by AMB+PMIM, AMB+MF, and PMIM+MF. Follow up period was 4 years after treatment. Cohorts were prospective except SSG (retrospective) and MF (partially retrospective). We compared incidence proportion and rate in 100-person-4year of PKDL and VLR by treatment regimens using univariate and multivariate analysis.
974 of 984 enrolled participants completed the study. Overall incidence proportion for PKDL and VLR was 12.3% (95% CI, 10.4%-14.5%) and 7.0% (95% CI, 5.6%-8.8%) respectively. The incidence rate (95% CI) of PKDL and VLR was 14.0 (8.6-22.7) and 7.6 (4.1-14.7) accordingly. SSG cohort had the lowest incidence rate of PKDL at 3.0 (1.3-7.3) and VLR at 1.8 (0.6-5.6), followed by MDAMB at 8.2 (4.3-15.7) for PKDL and at 2.7 (0.9-8.4) for VLR.
Development of PKDL and VLR is related with treatment regimens for VL. SSG and MDAMB resulted in less incidence of PKDL and VLR compared to other treatment regimens. MDAMB should be considered for VL as a first step for prevention of PKDL and VLR since SSG is highly toxic and not recommended for VL.
我们研究了内脏利什曼病(VL)治疗方案与卡拉-阿扎尔皮肤利什曼病(PKDL)和内脏利什曼病复发(VLR)发展之间的关系。
研究对象包括接受单药治疗(葡甲胺锑酸钠[SSG]、米替福新[MF]、肌肉内注射硫酸巴龙霉素[PMIM]、单剂量(SDAMB)和多剂量(MDAMB)脂质体两性霉素 B [AmBisome(AMB)])、AMB+PMIM、AMB+MF 和 PMIM+MF 联合治疗的 VL 治愈患者队列。随访期为治疗后 4 年。队列除 SSG(回顾性)和 MF(部分回顾性)外均为前瞻性。我们使用单变量和多变量分析比较了不同治疗方案 100 人-4 年的 PKDL 和 VLR 发生率比例和发生率。
984 名入组患者中有 974 名完成了研究。PKDL 和 VLR 的总发生率分别为 12.3%(95%CI,10.4%-14.5%)和 7.0%(95%CI,5.6%-8.8%)。PKDL 和 VLR 的发病率(95%CI)分别为 14.0(8.6-22.7)和 7.6(4.1-14.7)。SSG 队列的 PKDL 和 VLR 发生率最低,分别为 3.0(1.3-7.3)和 1.8(0.6-5.6),其次是 MDAMB,PKDL 发生率为 8.2(4.3-15.7),VLR 发生率为 2.7(0.9-8.4)。
PKDL 和 VLR 的发生与 VL 的治疗方案有关。与其他治疗方案相比,SSG 和 MDAMB 导致 PKDL 和 VLR 的发生率较低。由于 SSG 毒性很高,不建议用于 VL,因此 MDAMB 应作为预防 PKDL 和 VLR 的第一步,考虑用于 VL。