Swami Umang, Monga Varun, Bossler Aaron D, Zakharia Yousef, Milhem Mohammed
Division of Oncology, Department of Internal Medicine, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT, USA.
Division of Hematology, Oncology and Blood & Marrow Transplantation, University of Iowa Hospitals and Clinics, 200 Hawkins Dr., Iowa City, IA 52242, USA.
J Oncol. 2019 Jul 25;2019:1856594. doi: 10.1155/2019/1856594. eCollection 2019.
Anti-PD-1 therapies, pembrolizumab and nivolumab, are currently the standard of care for treatment of patients with metastatic melanoma. Treatment is usually continued until toxicity or disease progression. Though these therapies are well tolerated, some patients discontinue them due to immune-related adverse events (irAE). Discontinuation of therapy brings challenges to their management due to limited treatment options and lack of long-term prognostic information for these patients. Herein, we reviewed patients at our institution to analyze their clinical outcomes.
Charts of 1264 consecutive patients enrolled between 8/1/2012 and 7/31/2017 at Melanoma Skin & Ocular Tissue Repositories at Holden Comprehensive Cancer Center at the University of Iowa Hospitals and Clinic were reviewed. Eligible patients were those who received single-agent anti-PD-1 therapy and subsequently discontinued it due to irAE. Reviewed data included patient demographics, prior medical history, baseline disease parameters, and outcomes. Kaplan-Meier survival analysis was done to determine progression-free survival (PFS) and overall survival (OS).
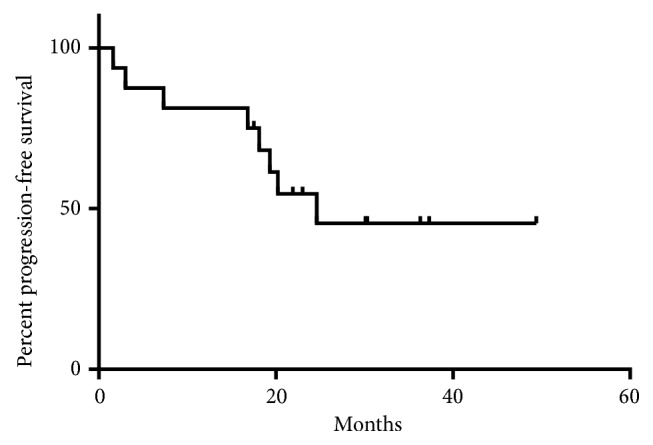
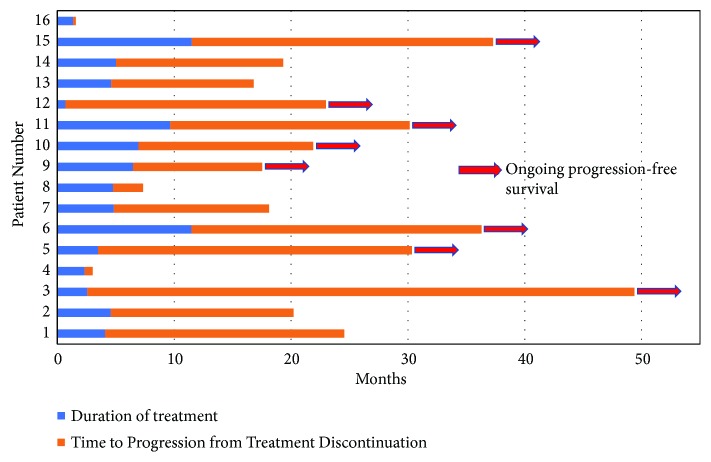
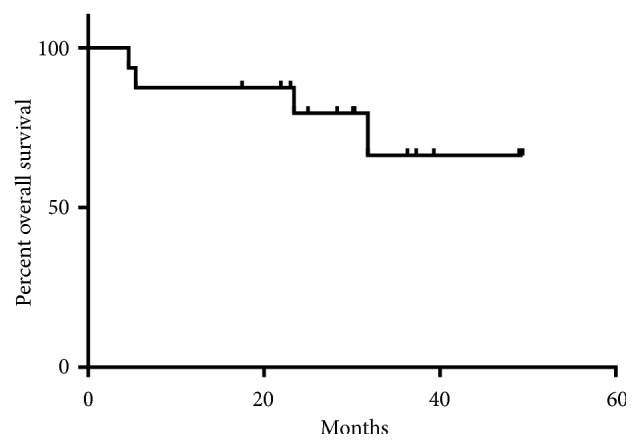
Overall 169 patients with advanced, unresectable, or metastatic cutaneous melanoma received anti-PD-1 therapy of which 16 (9.5%) white, non-Hispanic patients with median age of 64.5 (range 35 to 81 years) discontinued treatment due to irAE. Fifteen patients received pembrolizumab and one received nivolumab. The median duration of treatment was 4.7 (range 0.7 to 11.5) months. Median follow-up was 30.3 (range 4.6 to 49.4) months. Median PFS was 24.6 months and median OS was not reached. Durable clinical benefit (time to progression or next treatment of more than 6 months from last treatment) was observed in 13 (81.2%) patients. At the time of analysis, 8 patients had progressed and 4 patients died (all-cause).
Our results suggest that advanced melanoma patients discontinuing anti-PD-1 therapy due to irAE usually experience durable clinical benefit. However, caution is needed with these agents in patients with underlying autoimmune diseases.
抗程序性死亡蛋白1(PD-1)疗法帕博利珠单抗和纳武利尤单抗目前是转移性黑色素瘤患者治疗的标准方案。治疗通常持续进行,直至出现毒性反应或疾病进展。尽管这些疗法耐受性良好,但一些患者因免疫相关不良事件(irAE)而停药。由于治疗选择有限且缺乏这些患者的长期预后信息,停药给治疗管理带来了挑战。在此,我们回顾了我院的患者,以分析他们的临床结局。
回顾了2012年8月1日至2017年7月31日期间在爱荷华大学医院及诊所霍尔顿综合癌症中心黑色素瘤皮肤与眼部组织库连续入组的1264例患者的病历。符合条件的患者是那些接受单药抗PD-1治疗并随后因irAE停药的患者。回顾的数据包括患者人口统计学特征、既往病史、基线疾病参数和结局。采用Kaplan-Meier生存分析来确定无进展生存期(PFS)和总生存期(OS)。
总体而言,169例晚期、不可切除或转移性皮肤黑色素瘤患者接受了抗PD-1治疗,其中16例(9.5%)非西班牙裔白人患者因irAE停药,中位年龄为64.5岁(范围35至81岁)。15例患者接受了帕博利珠单抗治疗,1例接受了纳武利尤单抗治疗。中位治疗持续时间为4.7个月(范围0.7至11.5个月)。中位随访时间为30.3个月(范围4.6至49.4个月)。中位PFS为24.6个月,中位OS未达到。13例(81.2%)患者观察到持久的临床获益(自上次治疗起至疾病进展或接受下一次治疗的时间超过6个月)。在分析时,8例患者病情进展,4例患者死亡(各种原因)。
我们的结果表明,因irAE停用抗PD-1治疗的晚期黑色素瘤患者通常会有持久的临床获益。然而,对于患有潜在自身免疫性疾病的患者,使用这些药物时需要谨慎。