Center for Tropical Medicine and Global Health, University of Oxford Centre for Tropical Medicine, Oxford, UK
School of Cross Faculty Studies, University of Warwick, Coventry, UK.
BMJ Open. 2019 Aug 20;9(8):e028224. doi: 10.1136/bmjopen-2018-028224.
Low-income and middle-income countries (LMICs) are crucial in the global response to antimicrobial resistance (AMR), but diverse health systems, healthcare practices and cultural conceptions of medicine can complicate global education and awareness-raising campaigns. Social research can help understand LMIC contexts but remains under-represented in AMR research.
To (1) Describe antibiotic-related knowledge, attitudes and practices of the general population in two LMICs. (2) Assess the role of antibiotic-related knowledge and attitudes on antibiotic access from different types of healthcare providers.
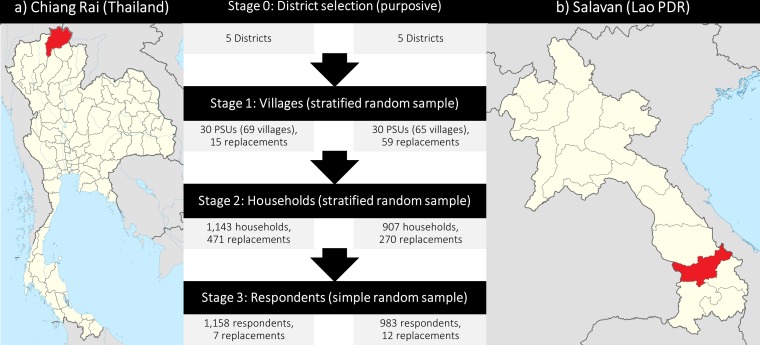
Observational study: cross-sectional rural health behaviour survey, representative of the population level.
General rural population in Chiang Rai (Thailand) and Salavan (Lao PDR), surveyed between November 2017 and May 2018.
2141 adult members (≥18 years) of the general rural population, representing 712 000 villagers.
Antibiotic-related knowledge, attitudes and practices across sites and healthcare access channels.
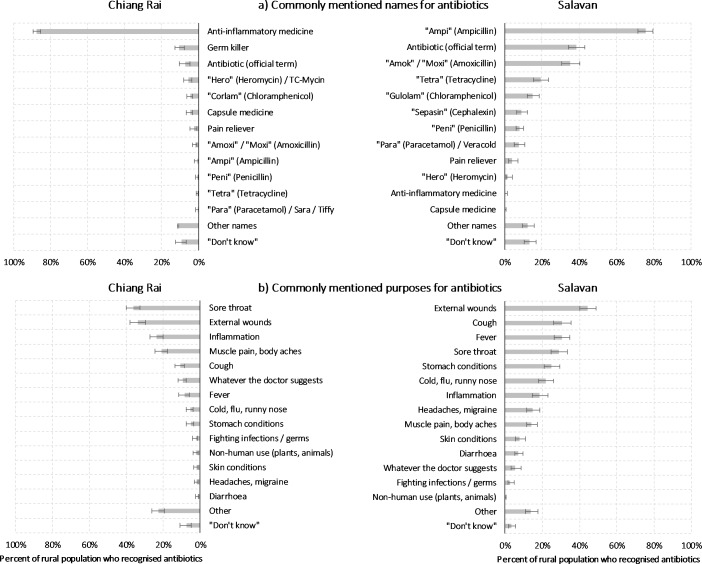
Villagers were aware of antibiotics (Chiang Rai: 95.7%; Salavan: 86.4%; p<0.001) and drug resistance (Chiang Rai: 74.8%; Salavan: 62.5%; p<0.001), but the usage of technical concepts for antibiotics was dwarfed by local expressions like 'anti-inflammatory medicine' in Chiang Rai (87.6%; 95% CI 84.9% to 90.0%) and in Salavan (75.6%; 95% CI 71.4% to 79.4%). Multivariate linear regression suggested that attitudes against over-the-counter antibiotics were linked to 0.12 additional antibiotic use episodes from public healthcare providers in Chiang Rai (95% CI 0.01 to 0.23) and 0.53 in Salavan (95% CI 0.16 to 0.90).
Locally specific conceptions and counterintuitive practices around antimicrobials can complicate AMR communication efforts and entail unforeseen consequences. Overcoming 'knowledge deficits' alone will therefore be insufficient for global AMR behaviour change. We call for an expansion of behavioural AMR strategies towards 'AMR-sensitive interventions' that address context-specific upstream drivers of antimicrobial use (eg, unemployment insurance) and complement education and awareness campaigns.
Clinicaltrials.gov identifier NCT03241316.
中低收入国家(LMICs)在全球对抗抗菌素耐药性(AMR)的反应中至关重要,但多样化的卫生系统、医疗保健实践和对医学的文化观念可能使全球教育和提高认识活动变得复杂。社会研究可以帮助了解 LMIC 背景,但在 AMR 研究中仍然代表性不足。
(1)描述两个 LMIC 中普通人群对抗生素相关知识、态度和实践的了解。(2)评估抗生素相关知识和态度对不同类型医疗保健提供者获取抗生素的影响。
观察性研究:横断面农村健康行为调查,代表人群水平。
泰国清莱和老挝沙拉湾的一般农村人口,于 2017 年 11 月至 2018 年 5 月间进行调查。
2141 名成年(≥18 岁)普通农村人口,代表 712000 名村民。
各地和各种医疗保健渠道的抗生素相关知识、态度和实践。
村民们了解抗生素(清莱:95.7%;沙拉湾:86.4%;p<0.001)和耐药性(清莱:74.8%;沙拉湾:62.5%;p<0.001),但抗生素的使用技术概念远不及当地的表达方式,如清莱的“消炎药”(87.6%;95%CI 84.9%至 90.0%)和沙拉湾的“消炎药”(75.6%;95%CI 71.4%至 79.4%)。多变量线性回归表明,对抗非处方抗生素的态度与清莱公共医疗保健提供者增加 0.12 次抗生素使用事件相关(95%CI 0.01 至 0.23),与沙拉湾增加 0.53 次抗生素使用事件相关(95%CI 0.16 至 0.90)。
围绕抗菌素的地方具体观念和违背直觉的做法可能使 AMR 沟通工作复杂化,并带来意想不到的后果。因此,仅克服“知识不足”不足以实现全球 AMR 行为改变。我们呼吁扩大行为 AMR 策略,以“对 AMR 敏感的干预措施”为重点,解决抗生素使用的特定于背景的上游驱动因素(例如,失业保险),并补充教育和提高认识活动。
Clinicaltrials.gov 标识符 NCT03241316。