The Jikei University School of Medicine, Department of Surgery, Division of Thoracic Surgery, Tokyo, Japan.
Thorac Cancer. 2019 Oct;10(10):1945-1952. doi: 10.1111/1759-7714.13173. Epub 2019 Aug 21.
Minimally invasive thoracoscopic lobectomy is the recommended surgery for clinical stage I non-small cell lung cancer (NSCLC). The purpose of this study was to identify the risk factors, including sarcopenia, for postoperative complications in patients undergoing a complete single-lobe thoracoscopic lobectomy for clinical stage I NSCLC, as well as the impact of complications on disease-free survival.
We retrospectively investigated 173 patients with pathologically-diagnosed NSCLC who underwent curative thoracoscopic lobectomies between April 2013 and March 2018. Sarcopenia was assessed using the psoas muscle index calculated from preoperative computed tomography images at the third lumbar vertebral level.
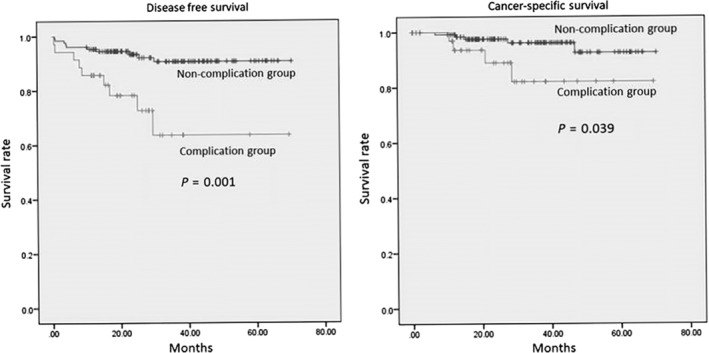
Complications developed in 38 (22%) patients, including 21 with prolonged air leak. In univariate analysis, the significant risk factors for complications were advanced age, male sex, higher Charlson Comorbidity Index (CCI) score, lower cholinesterase, lower albumin, higher creatinine level, pleural adhesion, operative time ≥ five hours, nonadenocarcinoma cancer, and larger tumor size. Multivariate analysis showed that age ≥ 75 years (P = 0.002) and pleural adhesion (P = 0.026) were significant independent risk factors for complications. Compared with the patient group without complications, postoperative complications were independently associated with shorter disease-free survival (P = 0.01).
Advanced age and pleural adhesion were independent risk factors for complications after complete single-lobe thoracoscopic lobectomies for clinical stage I NSCLC, and postoperative complications were statistically associated with poor prognosis. Surgical teams should ensure an experienced surgeon leads the operation for patients at higher risk to avoid prolonged postoperative hospitalization and a possible poor prognosis.
对于临床Ⅰ期非小细胞肺癌(NSCLC),微创胸腔镜肺叶切除术是推荐的手术方法。本研究旨在确定接受完全单肺叶胸腔镜肺叶切除术治疗临床Ⅰ期 NSCLC 患者的术后并发症的风险因素,包括肌少症,并探讨这些并发症对无病生存率的影响。
我们回顾性调查了 2013 年 4 月至 2018 年 3 月期间接受根治性胸腔镜肺叶切除术的 173 例病理诊断为 NSCLC 的患者。使用术前第 3 腰椎水平 CT 图像计算的腰大肌指数评估肌少症。
38 例(22%)患者发生了并发症,其中 21 例发生了长时间的气胸。单因素分析显示,并发症的显著危险因素包括高龄、男性、较高的 Charlson 合并症指数(CCI)评分、较低的胆碱酯酶、较低的白蛋白、较高的肌酐水平、胸膜粘连、手术时间≥5 小时、非腺癌、以及肿瘤较大。多因素分析显示,年龄≥75 岁(P = 0.002)和胸膜粘连(P = 0.026)是并发症的独立显著危险因素。与无并发症的患者组相比,术后并发症与无病生存率缩短独立相关(P = 0.01)。
高龄和胸膜粘连是临床Ⅰ期 NSCLC 患者完全单肺叶胸腔镜肺叶切除术后并发症的独立危险因素,术后并发症与不良预后有统计学关联。手术团队应为高风险患者安排经验丰富的外科医生进行手术,以避免术后长时间住院和可能的不良预后。