Ohnishi Takashi, Iwata Akira, Kanayama Masahiro, Oha Fumihiro, Hashimoto Tomoyuki, Iwasaki Norimasa
Spine Center, Hakodate Central General Hospital, Hokkaido, Japan.
Department of Orthopaedic Surgery, Faculty of Medicine and Graduate School of Medicine, Hokkaido University, Hokkaido, Japan.
Spine Surg Relat Res. 2018 Jan 27;2(1):72-76. doi: 10.22603/ssrr.2017-0046. eCollection 2018.
Numerous studies have reported the risk factors of osteoporotic vertebral collapse. However, whether spino-pelvic and global spinal alignments are associated with the occurrence of osteoporotic vertebral collapse remains unclear. This study aimed to investigate the association between spino-pelvic and global spinal alignments and the occurrence of osteoporotic vertebral collapse.
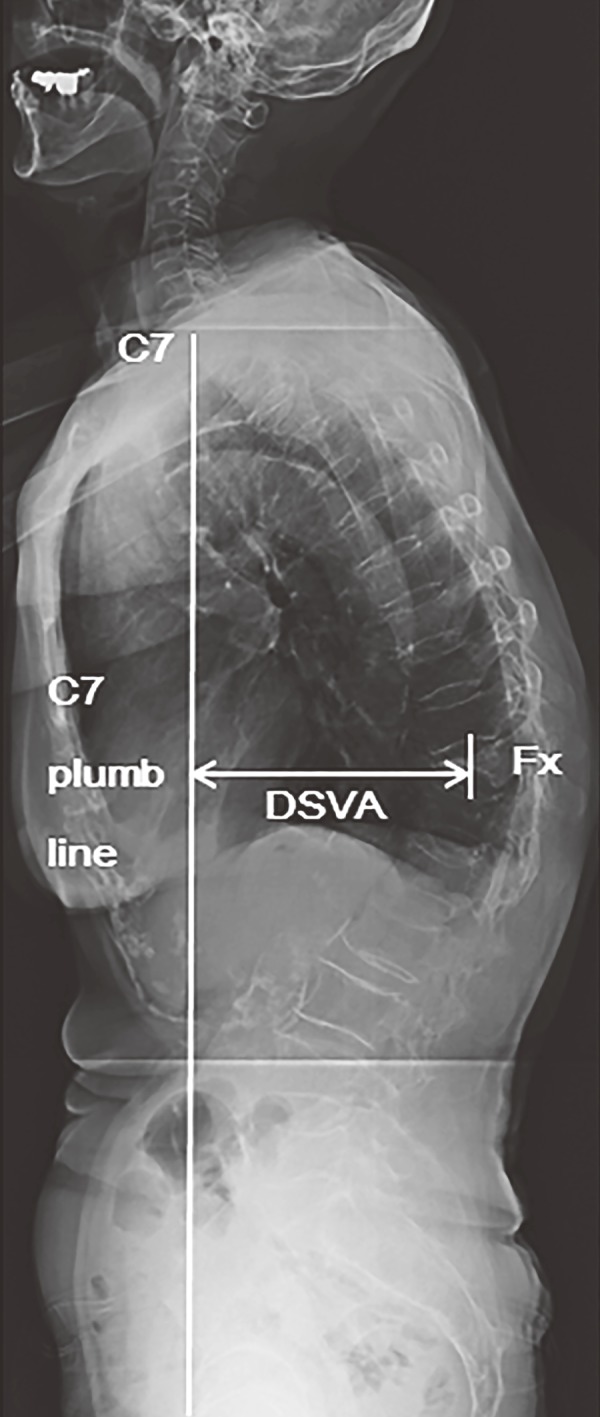
A total of 46 consecutive patients who underwent a nonoperative treatment for a single-level fresh osteoporotic thoracolumbar vertebral compression fracture (T10 to L3) were retrospectively reviewed. The parameters evaluated were the pelvic incidence, anterior deviation of the C7 plumb line, distance between the C7 plumb line and the center of the fractured vertebra, and kyphotic wedge angle of the fractured vertebra in a standing whole-spine radiograph at the beginning of the nonoperative treatment. As an outcome measure, the presence or absence of osteoporotic vertebral collapse was radiographically evaluated at the final follow-up. Multiple logistic regression analysis was used to determine significant risk factors of osteoporotic vertebral collapse.
The mean values for each parameter were as follows: pelvic incidence, 58.0 degrees; anterior deviation of the C7 plumb line, 3.0 cm; distance between the C7 plumb line and the center of the fractured vertebra, 5.7 cm; and kyphotic wedge angle of the fractured vertebra, 14.6 degrees. Multiple logistic regression analysis revealed that the distance between the C7 plumb line and center of the fractured vertebra was a significant risk factor of osteoporotic vertebral collapse (p = 0.012; odds ratio, 1.025). The anterior deviation of the C7 plumb line (p = 0.214), pelvic incidence (p = 0.728), and kyphotic wedge angle of the fractured vertebra (p = 0.07) did not affect the occurrence of osteoporotic vertebral collapse.
A large distance between the C7 plumb line and center of the fractured vertebra was a significant risk factor of osteoporotic vertebral collapse. The distance approximately represents that of between gravity center of trunk cranial to the fractured vertebra and the fractured vertebra. Accordingly, the large distance may cause larger flexion moment to the fractured site, leading to stress concentration that results in insufficient bone healing.
众多研究报告了骨质疏松性椎体塌陷的危险因素。然而,脊柱 - 骨盆及整体脊柱排列与骨质疏松性椎体塌陷的发生是否相关仍不清楚。本研究旨在探讨脊柱 - 骨盆及整体脊柱排列与骨质疏松性椎体塌陷发生之间的关联。
回顾性分析46例因单节段新鲜骨质疏松性胸腰椎椎体压缩骨折(T10至L3)接受非手术治疗的连续患者。评估的参数包括骨盆入射角、C7铅垂线的前向偏移、C7铅垂线与骨折椎体中心之间的距离,以及非手术治疗开始时站立位全脊柱X线片上骨折椎体的后凸楔角。作为结局指标,在最终随访时通过影像学评估骨质疏松性椎体塌陷的有无。采用多因素logistic回归分析确定骨质疏松性椎体塌陷的显著危险因素。
各参数的平均值如下:骨盆入射角58.0°;C7铅垂线的前向偏移3.0 cm;C7铅垂线与骨折椎体中心之间的距离5.7 cm;骨折椎体的后凸楔角14.6°。多因素logistic回归分析显示,C7铅垂线与骨折椎体中心之间的距离是骨质疏松性椎体塌陷的显著危险因素(p = 0.012;比值比,1.025)。C7铅垂线的前向偏移(p = 0.214)、骨盆入射角(p = 0.728)和骨折椎体的后凸楔角(p = 0.07)均不影响骨质疏松性椎体塌陷的发生。
C7铅垂线与骨折椎体中心之间的距离较大是骨质疏松性椎体塌陷的显著危险因素。该距离大致代表骨折椎体上方躯干重心与骨折椎体之间的距离。因此,该较大距离可能会给骨折部位带来更大的弯曲力矩,导致应力集中,从而造成骨愈合不足。