Department of Nephrology, Peking University Third Hospital, Beijing, China.
Division of Nephrology, Princess Alexandra Hospital, Brisbane, Australia.
PLoS One. 2019 Aug 23;14(8):e0221531. doi: 10.1371/journal.pone.0221531. eCollection 2019.
Clinical outcomes of patients with end-stage kidney disease (ESKD) secondary to membranous nephropathy (MN) have not been well described. This study aimed to evaluate patient and/or allograft outcomes of dialysis or kidney transplantation in patients with ESKD secondary to MN.
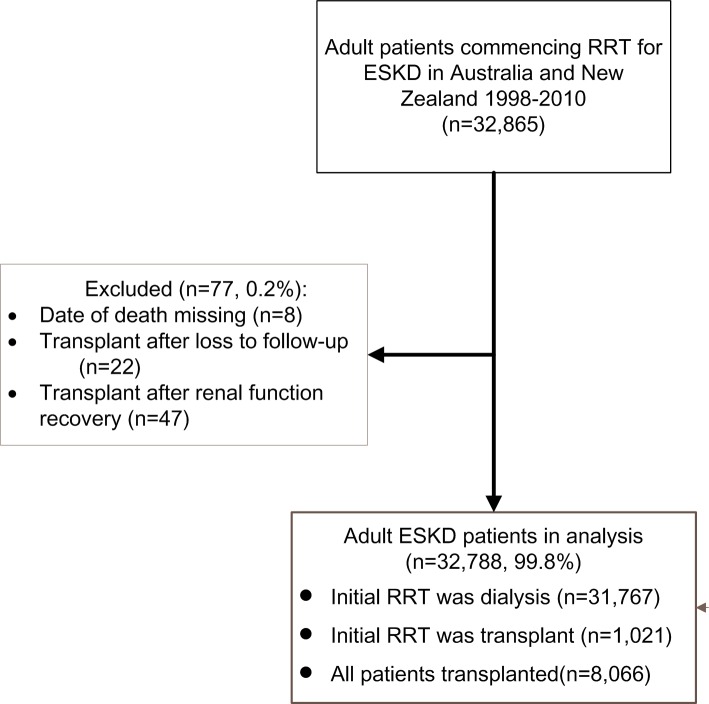
All adult patients with ESKD commencing renal replacement therapy in Australia and New Zealand from January 1998 to December 2010 were extracted retrospectively from ANZDATA registry on 31st December 2013. Outcomes of MN were compared to other causes of ESKD. In a secondary analysis, outcomes of MN were compared to all patients with ESKD due to other forms of glomerulonephritis.
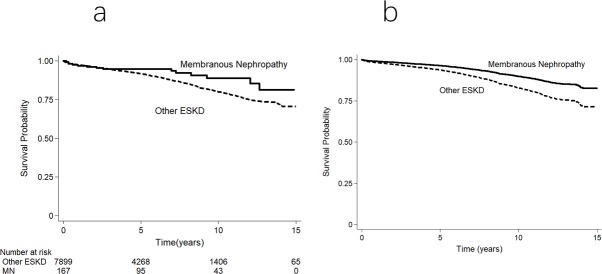
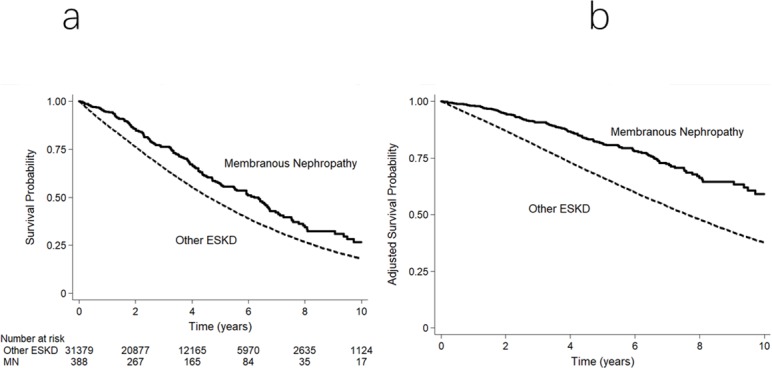
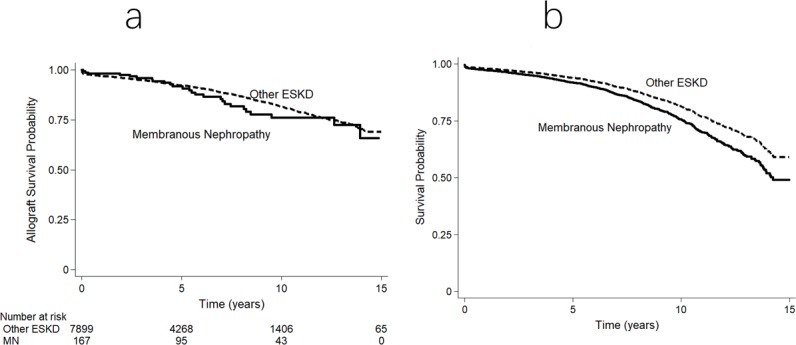
Of 32,788 included patients, 417 (1.3%) had MN. Compared to other causes of ESKD, MN experienced lower mortality on dialysis (adjusted hazard ratio [aHR] 0.79, 95% CI 0.68-0.92, p = 0.002) and following kidney transplantation (aHR 0.57, 95% CI 0.33-0.97, p = 0.04), had a higher risk of death-censored kidney allograft failure (aHR 1.55, 95% CI: 1.00-2.41, p = 0.05) but comparable risk of overall kidney allograft failure (aHR 1.35, 95% CI 0.91-2.01, p = 0.13). Similar results were obtained using competing-risk regression analyses. MN patients were significantly more likely to receive a kidney transplant (aHR 1.38, 95% CI 1.16-1.63, p<0.001) and to experience primary kidney disease recurrence in the allograft (aHR 4.92, 95% CI 3.02-8.01, p<0.001). Compared to other forms of glomerulonephritis, MN experienced comparable dialysis and transplant patient survival, but higher rates of kidney transplantation, primary renal disease recurrence and death-censored allograft failure.
MN was associated with superior survival on dialysis and following kidney transplantation compared to patients with other causes of ESKD, and comparable patient survival compared to patients with other forms of glomerulonephritis. However, patients with MN exhibited a higher rate of death-censored allograft loss as a result of primary kidney disease recurrence.
膜性肾病(MN)导致的终末期肾病(ESKD)患者的临床结局尚未得到很好的描述。本研究旨在评估透析或肾移植治疗 ESKD 合并 MN 患者的患者和/或移植物结局。
从 2013 年 12 月 31 日澳大利亚和新西兰的 ANZDATA 登记处回顾性提取了 1998 年 1 月至 2010 年 12 月期间开始接受肾脏替代治疗的所有成年 ESKD 患者。将 MN 的结果与其他 ESKD 病因进行比较。在二次分析中,将 MN 的结果与所有因其他形式的肾小球肾炎导致 ESKD 的患者进行了比较。
在纳入的 32788 名患者中,有 417 名(1.3%)患有 MN。与其他 ESKD 病因相比,MN 患者在透析时死亡率较低(校正后的危险比 [aHR] 0.79,95%CI 0.68-0.92,p=0.002),肾移植后死亡率也较低(aHR 0.57,95%CI 0.33-0.97,p=0.04),但发生死亡相关移植物失败的风险较高(aHR 1.55,95%CI:1.00-2.41,p=0.05),但总体移植物失败的风险相似(aHR 1.35,95%CI 0.91-2.01,p=0.13)。使用竞争风险回归分析也得到了类似的结果。MN 患者更有可能接受肾移植(aHR 1.38,95%CI 1.16-1.63,p<0.001),并且在移植物中更易发生原发性肾脏疾病复发(aHR 4.92,95%CI 3.02-8.01,p<0.001)。与其他形式的肾小球肾炎相比,MN 患者在透析和移植患者的生存率方面相当,但肾移植、原发性肾脏疾病复发和死亡相关移植物失败的发生率更高。
与其他 ESKD 病因患者相比,MN 患者在透析和肾移植后生存率更高,与其他形式的肾小球肾炎患者的生存率相当。然而,MN 患者因原发性肾脏疾病复发而导致死亡相关移植物丧失的发生率更高。