Department of Urology, University of California, San Francisco, Helen Diller Family Comprehensive Cancer Center, San Francisco, CA, USA.
Department of Urology, Ludwig-Maximilians-University Munich, Munich, Germany.
Prostate Cancer Prostatic Dis. 2020 Mar;23(1):136-143. doi: 10.1038/s41391-019-0167-9. Epub 2019 Aug 27.
We aimed to validate Decipher to predict adverse pathology (AP) at radical prostatectomy (RP) in men with National Comprehensive Cancer Network (NCCN) favorable-intermediate risk (F-IR) prostate cancer (PCa), and to better select F-IR candidates for active surveillance (AS).
In all, 647 patients diagnosed with NCCN very low/low risk (VL/LR) or F-IR prostate cancer were identified from a multi-institutional PCa biopsy database; all underwent RP with complete postoperative clinicopathological information and Decipher genomic risk scores. The performance of all risk assessment tools was evaluated using logistic regression model for the endpoint of AP, defined as grade group 3-5, pT3b or higher, or lymph node invasion.
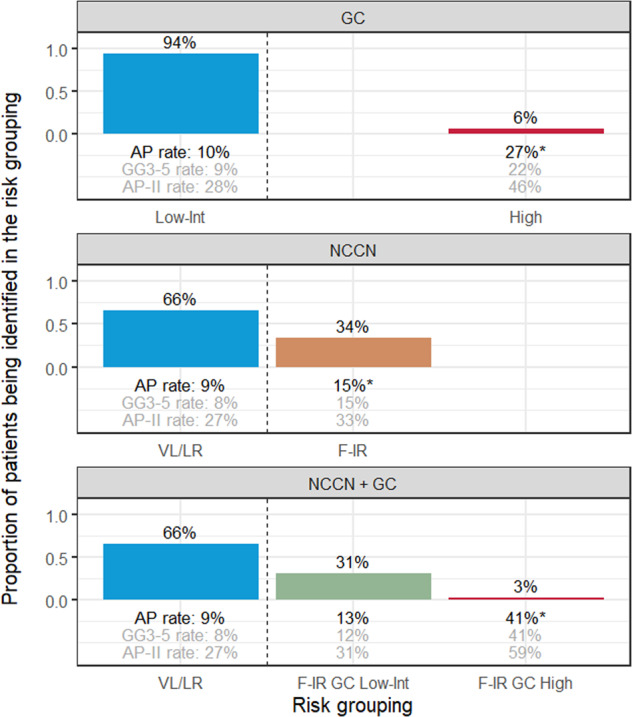
The median age was 61 years (interquartile range 56-66) for 220 patients with NCCN F-IR disease, 53% classified as low-risk by Cancer of the Prostate Risk Assessment (CAPRA 0-2) and 47% as intermediate-risk (CAPRA 3-5). Decipher classified 79%, 13% and 8% of men as low-, intermediate- and high-risk with 13%, 10%, and 41% rate of AP, respectively. Decipher was an independent predictor of AP with an odds ratio of 1.34 per 0.1 unit increased (p value = 0.002) and remained significant when adjusting by CAPRA. Notably, F-IR with Decipher low or intermediate score did not associate with significantly higher odds of AP compared to VL/LR.
NCCN risk groups, including F-IR, are highly heterogeneous and should be replaced with multivariable risk-stratification. In particular, incorporating Decipher may be useful for safely expanding the use of AS in this patient population.
我们旨在验证 Decipher 模型预测接受根治性前列腺切除术(RP)治疗的美国国家综合癌症网络(NCCN)中低危-中危(F-IR)前列腺癌(PCa)患者术后发生不良病理(AP)的能力,并更好地选择 F-IR 患者进行主动监测(AS)。
从多机构前列腺癌活检数据库中纳入 647 例诊断为 NCCN 极低危/低危(VL/LR)或 F-IR PCa 的患者,所有患者均接受 RP 治疗,并具有完整的术后临床病理资料和 Decipher 基因组风险评分。使用逻辑回归模型评估所有风险评估工具对 AP 终点(定义为组织学分级 3-5 级、pT3b 及以上或淋巴结侵犯)的预测性能。
220 例 NCCN F-IR 疾病患者的中位年龄为 61 岁(四分位距 56-66),53%的患者根据前列腺癌风险评估(CAPRA 0-2)分类为低危,47%为中危。Decipher 将 79%、13%和 8%的男性分别分类为低危、中危和高危,AP 发生率分别为 13%、10%和 41%。Decipher 是 AP 的独立预测因素,每增加 0.1 个单位,优势比为 1.34(p 值=0.002),调整 CAPRA 后仍然具有统计学意义。值得注意的是,与 VL/LR 相比,F-IR 患者中 Decipher 低或中评分与 AP 发生率显著升高无关。
NCCN 风险分组,包括 F-IR,高度异质,应采用多变量风险分层替代。特别是,纳入 Decipher 可能有助于安全扩大该患者群体中 AS 的应用。