Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine, Beijing Key Laboratory of Respiratory and Pulmonary Circulation Disorders, Beijing Engineering Research Center for Diagnosis and Treatment of Pulmonary and Critical Care, Beijing Chao-Yang Hospital, Capital Medical University, No. 8 Gongren Tiyuchang Nanlu, Chaoyang District, Beijing, 100020, China.
Department of Respiratory and Critical Care Medicine, Beijing Hospital, Beijing, China.
Crit Care. 2019 Sep 4;23(1):300. doi: 10.1186/s13054-019-2575-6.
Our pilot study suggested that noninvasive ventilation (NIV) reduced the need for intubation compared with conventional administration of oxygen on patients with "early" stage of mild acute respiratory distress syndrome (ARDS, PaO/FIO between 200 and 300).
To evaluate whether early NIV can reduce the need for invasive ventilation in patients with pneumonia-induced early mild ARDS.
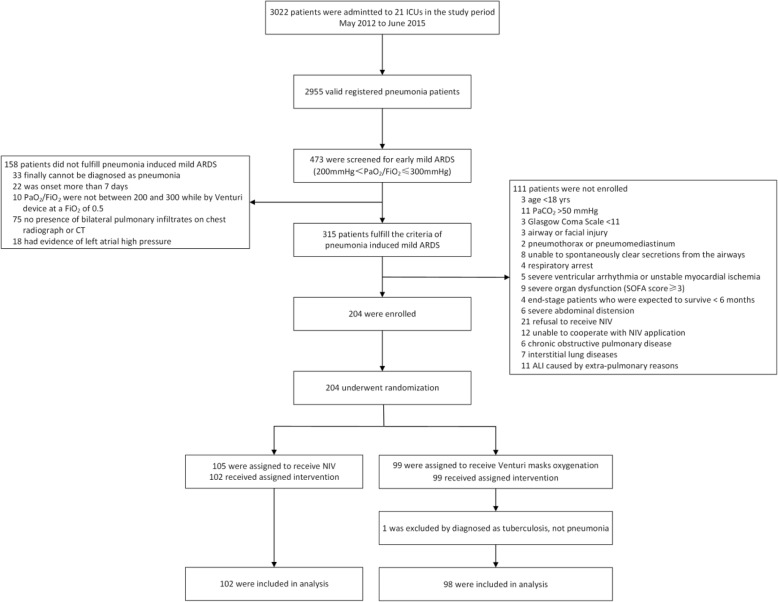
Prospective, multicenter, randomized controlled trial (RCT) of NIV compared with conventional administration of oxygen through a Venturi mask. Primary outcome included the numbers of patients who met the intubation criteria.
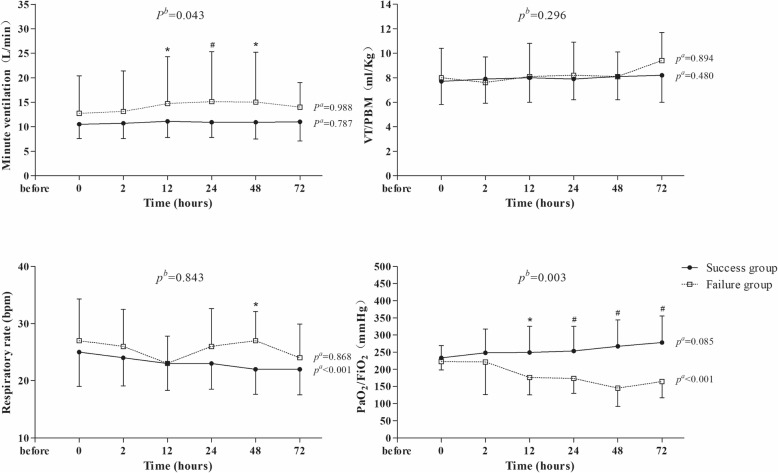
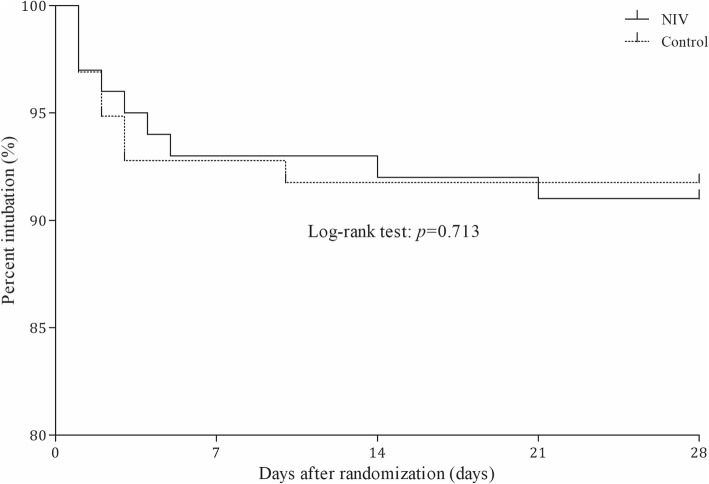
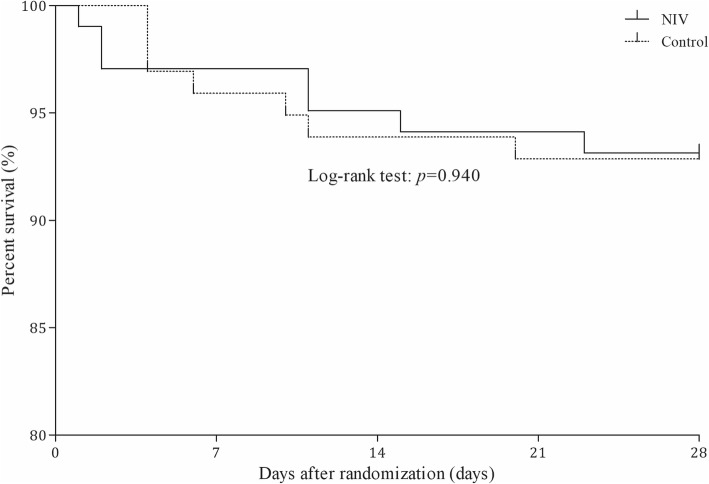
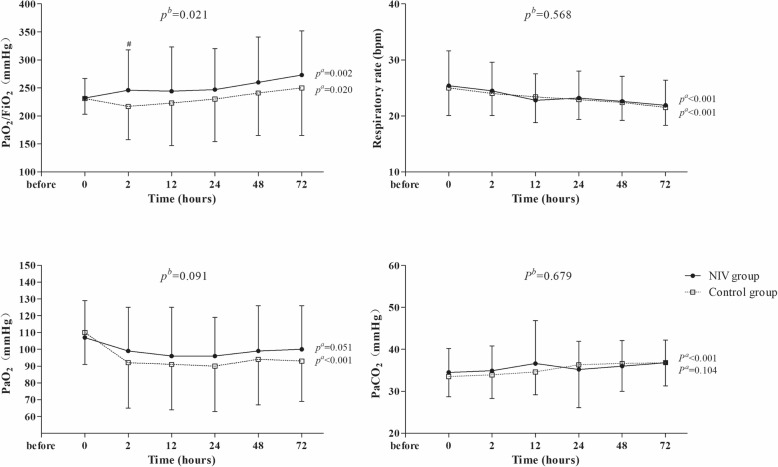
Two hundred subjects were randomized to NIV (n = 102) or control (n = 98) groups from 21 centers. Baseline characteristics were similar in the two groups. In the NIV group, PaO/FIO became significantly higher than in the control group at 2 h after randomization and remained stable for the first 72 h. NIV did not decrease the proportion of patients requiring intubation than in the control group (11/102 vs. 9/98, 10.8% vs. 9.2%, p = 0.706). The ICU mortality was similar in the two groups (7/102 vs. 7/98, 4.9% vs. 3.1%, p = 0.721). Multivariate analysis showed minute ventilation greater than 11 L/min at 48 h was the independent risk factor for NIV failure (OR, 1.176 [95% CI, 1.005-1.379], p = 0.043).
Treatment with NIV did not reduce the need for intubation among patients with pneumonia-induced early mild ARDS, despite the improved PaO/FIO observed with NIV compared with standard oxygen therapy. High minute ventilation may predict NIV failure.
NCT01581229 . Registered 19 April 2012.
我们的初步研究表明,与常规吸氧相比,无创通气(NIV)可降低“早期”轻度急性呼吸窘迫综合征(ARDS,PaO/FIO 在 200 至 300 之间)患者的插管需求。
评估早期 NIV 是否可降低肺炎所致早期轻度 ARDS 患者的有创通气需求。
前瞻性、多中心、随机对照试验(RCT),比较 NIV 与经文丘里面罩常规给氧。主要结局包括符合插管标准的患者人数。
21 个中心的 200 例患者被随机分配至 NIV(n=102)或对照组(n=98)。两组患者的基线特征相似。NIV 组患者随机分组后 2 小时 PaO/FIO 显著高于对照组,并在最初 72 小时内保持稳定。与对照组相比,NIV 并未降低需要插管的患者比例(11/102 比 9/98,10.8%比 9.2%,p=0.706)。两组患者 ICU 死亡率相似(7/102 比 7/98,4.9%比 3.1%,p=0.721)。多变量分析显示,48 小时时分钟通气量大于 11L/min 是 NIV 失败的独立危险因素(OR,1.176[95%CI,1.005-1.379],p=0.043)。
尽管与标准氧疗相比,NIV 可改善 PaO/FIO,但 NIV 治疗并未降低肺炎所致早期轻度 ARDS 患者的插管需求。高分钟通气量可能预示着 NIV 失败。
NCT01581229。于 2012 年 4 月 19 日注册。