Department of Anesthesiology, Critical Care and Pain Medicine, Division of Critical Care Medicine, Boston Children's Hospital, Harvard Medical School, Boston, Massachusetts, USA
The Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health and NIHR Great Ormond Street Hospital Biomedical Research Centre, London, UK.
Arch Dis Child. 2020 Apr;105(4):332-338. doi: 10.1136/archdischild-2019-317910. Epub 2019 Sep 4.
Individuals with X-linked myotubular myopathy (XLMTM) who survive infancy require extensive supportive care, including ventilator assistance, wheelchairs and feeding tubes. Half die before 18 months of age. We explored respiratory support and associated mortality risk in RECENSUS, particularly among patients ≤5 years old who received respiratory support at birth; this subgroup closely matches patients in the ASPIRO trial of gene therapy for XLMTM.
RECENSUS is an international, retrospective study of patients with XLMTM. Descriptive and time-to-event analyses examined survival on the basis of age, respiratory support, tracheostomy use, predicted mutational effects and life-sustaining care.
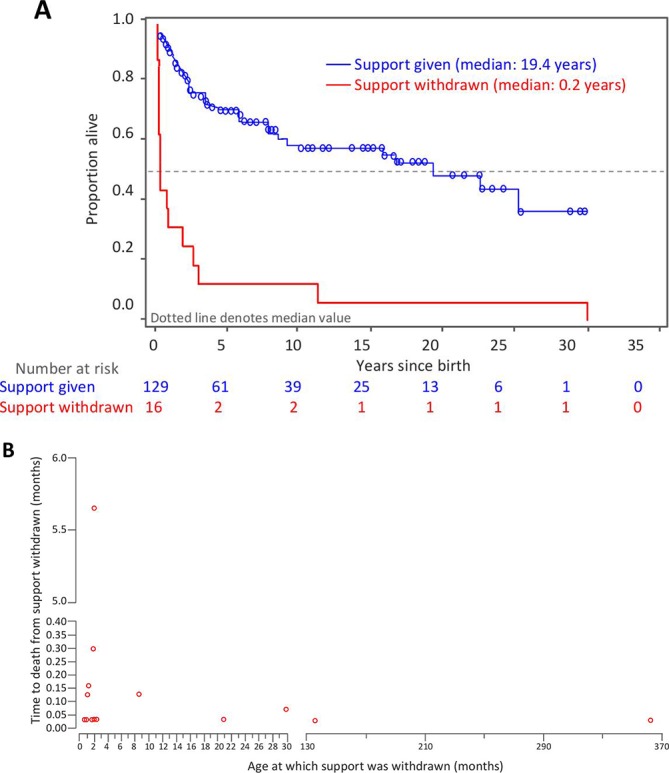
Outcomes for 145 patients were evaluated. Among 126 patients with respiratory support at birth, mortality was 47% overall and 59% among those ≤5 years old. Median survival time was shorter for patients ≤5 years old than for those >5 years old (2.2 years (IQR 0.7-5.6) vs 30.2 years (IQR 19.4-30.2)). The most common cause of death was respiratory failure (66.7%). Median survival time was longer for patients with a tracheostomy than for those without (22.8 years (IQR 8.7-30.2) vs 1.8 years (IQR 0.2-not estimable)). The proportion of patients living without a tracheostomy was 50% at age 6 months and 28% at age 2 years. Median survival time was longer with provision of life-sustaining care than without (19.4 years (IQR 3.1-not estimable) vs 0.2 years (IQR 0.1-2.1)).
High mortality, principally due to respiratory failure, among patients with XLMTM ≤5 years old despite respiratory support underscores the need for early diagnosis, informed decision-making and disease-modifying therapies.
NCT02231697.
患有 X 连锁肌小管肌病(XLMTM)的个体在婴儿期后需要广泛的支持性护理,包括呼吸机辅助、轮椅和喂养管。有一半的患者在 18 个月之前死亡。我们在 RECENSUS 中研究了呼吸支持及其相关的死亡风险,特别是在出生时接受呼吸支持的≤5 岁患者中;这个亚组与 XLMTM 基因治疗的 ASPIRO 试验中的患者非常匹配。
RECENSUS 是一项针对 XLMTM 患者的国际回顾性研究。描述性和时间事件分析根据年龄、呼吸支持、气管造口术使用、预测突变效应和维持生命的治疗来检查生存情况。
评估了 145 名患者的结局。在 126 名出生时接受呼吸支持的患者中,总体死亡率为 47%,≤5 岁的患者死亡率为 59%。≤5 岁患者的中位生存时间短于>5 岁患者(2.2 年(IQR 0.7-5.6)与 30.2 年(IQR 19.4-30.2))。最常见的死亡原因是呼吸衰竭(66.7%)。有气管造口术的患者中位生存时间长于无气管造口术的患者(22.8 年(IQR 8.7-30.2)与 1.8 年(IQR 0.2-不可估计))。6 个月时无需气管造口术的患者比例为 50%,2 岁时为 28%。提供维持生命的治疗比不提供维持生命的治疗中位生存时间更长(19.4 年(IQR 3.1-不可估计)与 0.2 年(IQR 0.1-2.1))。
尽管提供了呼吸支持,但≤5 岁的 XLMTM 患者死亡率高,主要是由于呼吸衰竭,这突显了早期诊断、知情决策和疾病修饰治疗的必要性。
NCT02231697。