Boston Children's Hospital, Harvard Medical School, Boston, MA, USA.
Hospital for Sick Children, University of Toronto, Toronto, ON, Canada.
Respir Res. 2024 Sep 16;25(1):342. doi: 10.1186/s12931-024-02966-0.
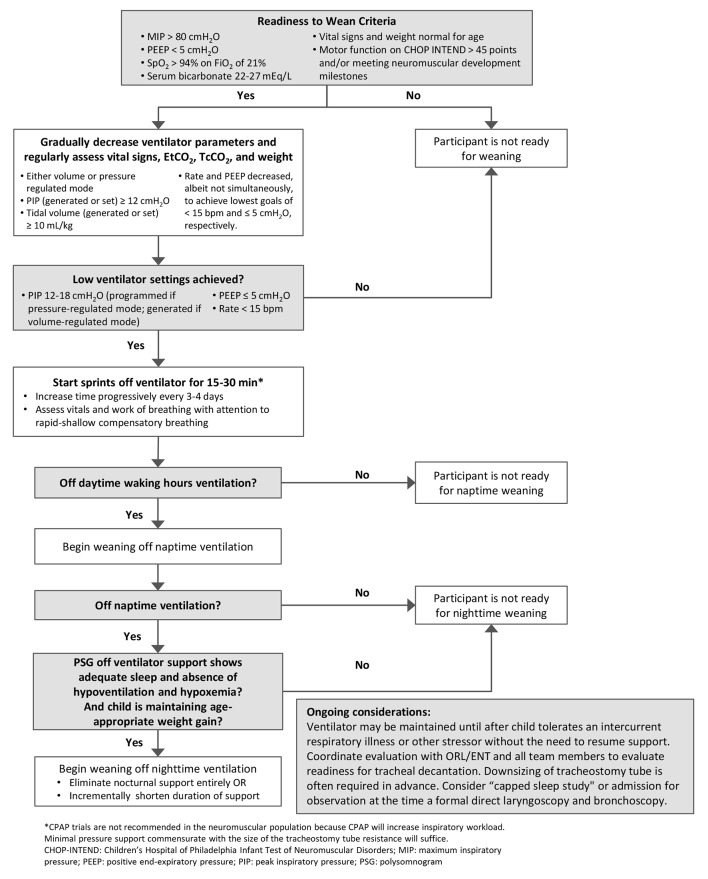
X-linked myotubular myopathy (XLMTM) is a rare, life-threatening congenital myopathy. Most (80%) children with XLMTM have profound muscle weakness and hypotonia at birth resulting in severe respiratory insufficiency, the inability to sit up, stand or walk, and early mortality. At birth, 85-90% of children with XLMTM require mechanical ventilation, with more than half requiring invasive ventilator support. Historically, ventilator-dependent children with neuromuscular-derived respiratory failure of this degree and nature, static or progressive, are not expected to achieve complete independence from mechanical ventilator support. In the ASPIRO clinical trial (NCT03199469), participants receiving a single intravenous dose of an investigational gene therapy (resamirigene bilparvovec) started showing significant improvements in daily hours of ventilation support compared with controls by 24 weeks post-dosing, and 16 of 24 dosed participants achieved ventilator independence between 14 and 97 weeks after dosing. At the time, there was no precedent or published guidance for weaning chronically ventilated children with congenital neuromuscular diseases off mechanical ventilation. When the first ASPIRO participants started showing dramatically improved respiratory function, the investigators initiated efforts to safely wean them off ventilator support, in parallel with primary protocol respiratory outcome measures. A group of experts in respiratory care and physiology and management of children with XLMTM developed an algorithm to safely wean children in the ASPIRO trial off mechanical ventilation as their respiratory muscle strength increased. The algorithm developed for this trial provides recommendations for assessing weaning readiness, a stepwise approach to weaning, and monitoring of children during and after the weaning process.
X 连锁肌小管肌病(XLMTM)是一种罕见的危及生命的先天性肌病。大多数(80%)XLMTM 患儿出生时即存在严重的肌肉无力和低张力,导致严重的呼吸功能不全、无法坐立、站立或行走,以及早期死亡。出生时,85-90%的 XLMTM 患儿需要机械通气,其中一半以上需要有创呼吸机支持。历史上,具有这种程度和性质的神经肌肉源性呼吸衰竭、静态或进行性的呼吸机依赖儿童,预计无法完全脱离机械通气支持。在 ASPIRO 临床试验(NCT03199469)中,接受单次静脉注射研究性基因治疗(resamirigene bilparvovec)的参与者在给药后 24 周与对照组相比,每日通气支持时间显著改善,并且 24 名给药参与者中有 16 名在给药后 14 至 97 周之间实现了呼吸机独立性。当时,对于患有先天性神经肌肉疾病的慢性通气儿童,尚无脱机的先例或已发表的指南。当第一批 ASPIRO 参与者开始显示出呼吸功能显著改善时,研究人员开始努力安全地为他们脱机,同时与主要方案的呼吸结局测量并行。一组呼吸护理和生理学以及 XLMTM 患儿管理方面的专家制定了一个算法,以安全地为 ASPIRO 试验中的儿童脱机,因为他们的呼吸肌力量增加。该试验中制定的算法为评估脱机准备情况、逐步脱机方法以及在脱机过程中和脱机后监测儿童提供了建议。