Blumenfeld Zeev
Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel.
Clin Med Insights Reprod Health. 2019 Aug 21;13:1179558119870163. doi: 10.1177/1179558119870163. eCollection 2019.
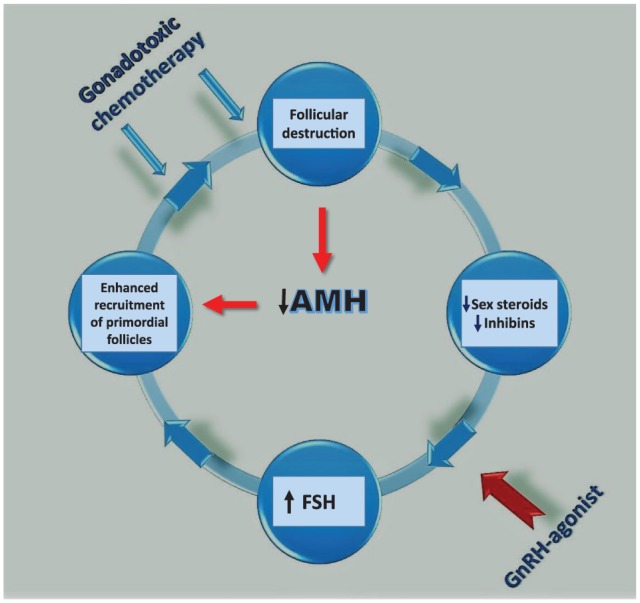
The only clinically accepted method of fertility preservation in young women facing gonadotoxic chemo- and/or radiotherapy for malignant or autoimmune diseases is cryopreservation of embryos or unfertilized ova, whereas cryopreservation of ovarian tissue for future reimplantation, or in vitro maturation of follicles, and the use of gonadotropin-releasing hormone agonists (GnRHa) are still considered investigational, by several authorities. Whereas previous publications have raised the fear of GnRHa's possible detrimental effects in patients with hormone receptor-positive breast cancers, recent randomized controlled trials (RCTs) have shown that it either improves or does not affect disease-free survival (DFS) in such patients. This review summarizes the pros and cons of GnRHa co-treatment for fertility preservation, suggesting 5 theoretical mechanisms for GnRHa action: (1) simulating the prepubertal hypogonadotropic milieu, (2) direct effect on GnRH receptors, (3) decreased ovarian perfusion, (4) upregulation of an ovarian-protecting molecule such as sphingosine-1-phosphate, and (5) protecting a possible germinative stem cell. We try to explain the reasons for the discrepancy between most publications that support the use of GnRHa for fertility preservation and the minority of publications that did not support its efficiency.
对于面临因恶性疾病或自身免疫性疾病而接受性腺毒性化疗和/或放疗的年轻女性,目前临床上唯一被认可的生育力保存方法是冷冻胚胎或未受精的卵子,而将卵巢组织冷冻以备将来移植、卵泡的体外成熟以及使用促性腺激素释放激素激动剂(GnRHa)仍被多个权威机构视为试验性方法。尽管先前的出版物引发了对GnRHa可能对激素受体阳性乳腺癌患者产生有害影响的担忧,但最近的随机对照试验(RCT)表明,它要么改善要么不影响此类患者的无病生存期(DFS)。本综述总结了GnRHa联合治疗用于生育力保存的利弊,提出了GnRHa作用的5种理论机制:(1)模拟青春期前低促性腺激素环境,(2)对GnRH受体的直接作用,(3)降低卵巢灌注,(4)上调卵巢保护分子如鞘氨醇-1-磷酸,以及(5)保护可能的生殖干细胞。我们试图解释大多数支持使用GnRHa进行生育力保存的出版物与少数不支持其有效性的出版物之间存在差异的原因。