Stroke Research Centre, Institute of Neurology, University College London, Russell Square House, 10 Russell Square, London, UK.
Stroke Center and Neurology, Department of Clinical Research, University Hospital and University, Basel, Switzerland.
J Neurol. 2019 Dec;266(12):3126-3135. doi: 10.1007/s00415-019-09536-1. Epub 2019 Sep 20.
To obtain precise estimates of age, haematoma volume, secondary haematoma expansion (HE) and mortality for patients with intracerebral haemorrhage (ICH) taking oral anticoagulants [Vitamin K antagonists (VKA-ICH) or non-Vitamin K antagonist oral anticoagulants (NOAC-ICH)] and those not taking oral anticoagulants (non-OAC ICH) at ICH symptom onset.
We conducted a systematic review and meta-analysis of studies comparing VKA-ICH or NOAC-ICH or both with non-OAC ICH. Primary outcomes were haematoma volume (in ml), HE, and mortality (in-hospital and 3-month). We calculated odds ratios (ORs) using the Mantel-Haenszel random-effects method and corresponding 95% confidence intervals (95%CI) and determined the mean ICH volume difference.
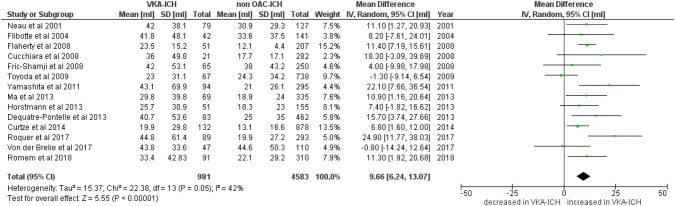
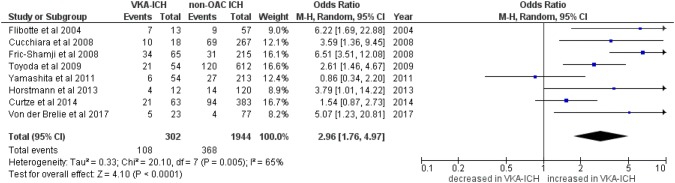
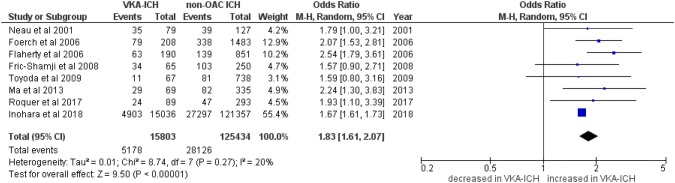
We identified 19 studies including data from 16,546 patients with VKA-ICH and 128,561 patients with non-OAC ICH. Only 2 studies reported data on 4943 patients with NOAC-ICH. Patients with VKA-ICH were significantly older than patients with non-OAC ICH (mean age difference: 5.55 years, 95%CI 4.03-7.07, p < 0.0001, I = 92%, p < 0.001). Haematoma volume was significantly larger in VKA-ICH with a mean difference of 9.66 ml (95%CI 6.24-13.07 ml, p < 0.00001; I = 42%, p = 0.05). HE occurred significantly more often in VKA-ICH (OR 2.96, 95%CI 1.74-4.97, p < 0.00001; I = 65%). VKA-ICH was associated with significantly higher in-hospital mortality (VKA-ICH: 32.8% vs. non-OAC ICH: 22.4%; OR 1.83, 95%CI 1.61-2.07, p < 0.00001, I = 20%, p = 0.27) and 3-month mortality (VKA-ICH: 47.1% vs. non-OAC ICH: 25.5%; OR 2.24, 95%CI 1.52-3.31, p < 0.00001, I = 71%, p = 0.001). We did not find sufficient data for a meta-analysis comparing NOAC-ICH and non-OAC-ICH.
This meta-analysis confirms, refines and expands findings from prior studies. We provide precise estimates of key prognostic factors and outcomes for VKA-ICH, which has larger haematoma volume, increased rate of HE and higher mortality compared to non-OAC ICH. There are insufficient data on NOACs.
针对脑出血(ICH)发病时服用口服抗凝剂[维生素 K 拮抗剂(VKA-ICH)或非维生素 K 拮抗剂口服抗凝剂(NOAC-ICH)]和未服用口服抗凝剂(非-OAC ICH)的患者,准确估计其年龄、血肿体积、继发性血肿扩大(HE)和死亡率。
我们对比较 VKA-ICH 或 NOAC-ICH 或两者与非-OAC ICH 的研究进行了系统评价和荟萃分析。主要结局是血肿体积(ml)、HE 和死亡率(住院期间和 3 个月)。我们使用 Mantel-Haenszel 随机效应法和相应的 95%置信区间(95%CI)计算比值比(OR),并确定平均 ICH 体积差异。
我们确定了 19 项研究,包括来自 16546 例 VKA-ICH 患者和 128561 例非-OAC ICH 患者的数据。只有 2 项研究报告了 4943 例 NOAC-ICH 患者的数据。VKA-ICH 患者明显比非-OAC ICH 患者年龄大(平均年龄差异:5.55 岁,95%CI 4.03-7.07,p<0.0001,I=92%,p<0.001)。VKA-ICH 的血肿体积明显更大,平均差异为 9.66ml(95%CI 6.24-13.07ml,p<0.00001;I=42%,p=0.05)。VKA-ICH 中 HE 发生的频率明显更高(OR 2.96,95%CI 1.74-4.97,p<0.00001;I=65%)。VKA-ICH 与更高的住院死亡率(VKA-ICH:32.8% vs. 非-OAC ICH:22.4%;OR 1.83,95%CI 1.61-2.07,p<0.00001,I=20%,p=0.27)和 3 个月死亡率(VKA-ICH:47.1% vs. 非-OAC ICH:25.5%;OR 2.24,95%CI 1.52-3.31,p<0.00001,I=71%,p=0.001)相关。我们没有找到足够的数据进行比较 NOAC-ICH 和非-OAC-ICH 的荟萃分析。
本荟萃分析证实、完善和扩展了既往研究的发现。我们提供了 VKA-ICH 关键预后因素和结局的准确估计值,与非-OAC ICH 相比,VKA-ICH 的血肿体积更大、HE 发生率更高、死亡率更高。关于 NOAC 的数据不足。