Hospital Universitario Fundación Alcorcón, Alcorcón, Madrid, Spain.
Hospital de Basurto, Vizcaya, Spain.
Cancer Med. 2019 Nov;8(16):6955-6966. doi: 10.1002/cam4.2555. Epub 2019 Oct 1.
Consensus is lacking regarding the optimal salvage therapy for patients with follicular lymphoma who relapse after or are refractory to immunochemotherapy.
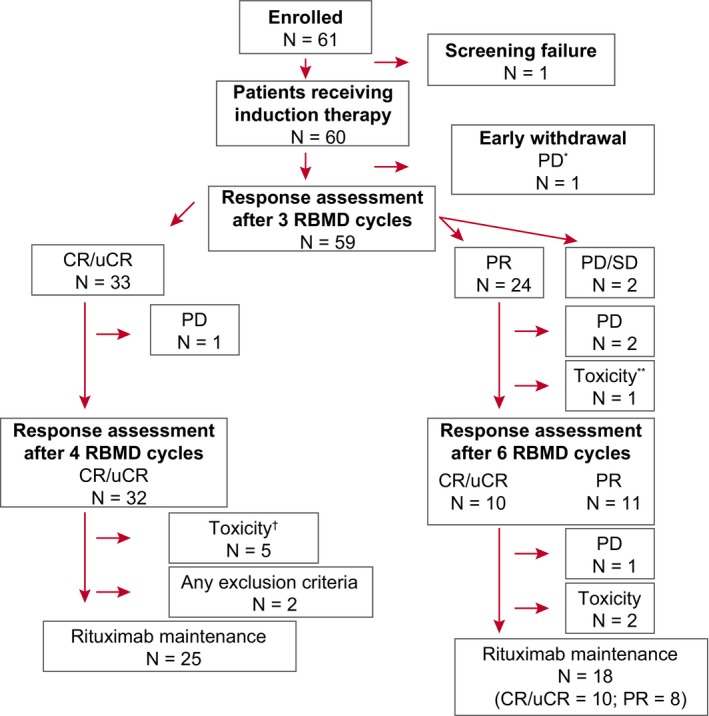
This phase II trial evaluated the efficacy and safety of response-adapted therapy with rituximab, bendamustine, mitoxantrone, and dexamethasone (RBMD) in follicular lymphoma patients who relapsed after or were refractory to first-line immunochemotherapy. Sixty patients received three treatment cycles, and depending on their response received an additional one (complete/unconfirmed complete response) or three (partial response) cycles. Patients who responded to induction received rituximab maintenance therapy for 2 years.
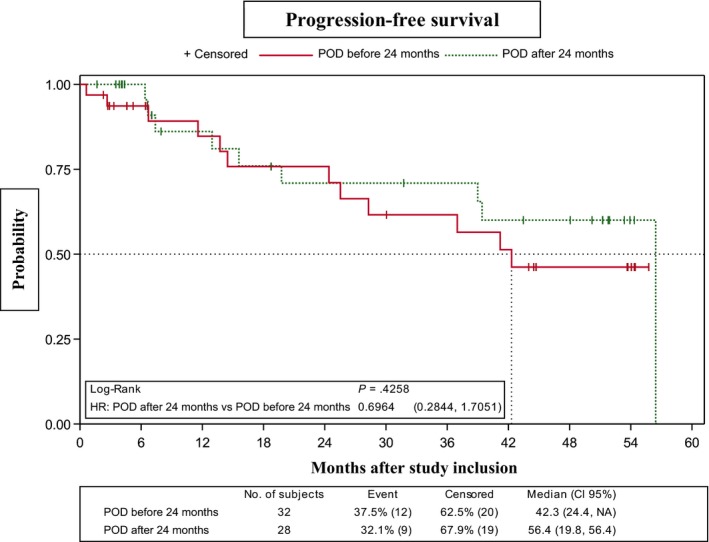
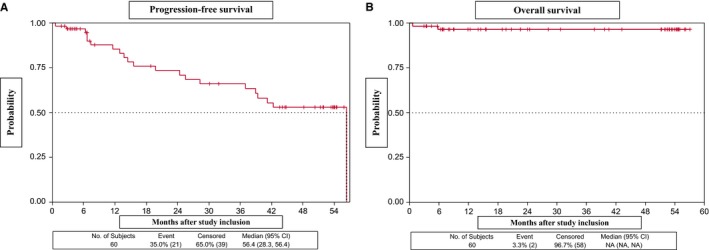
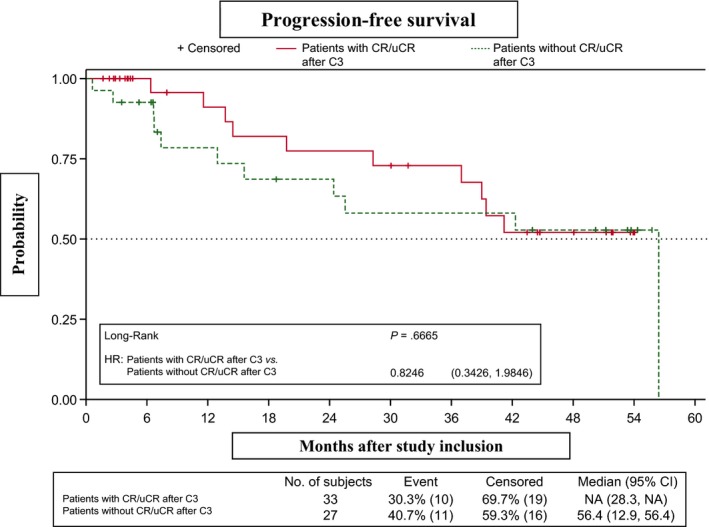
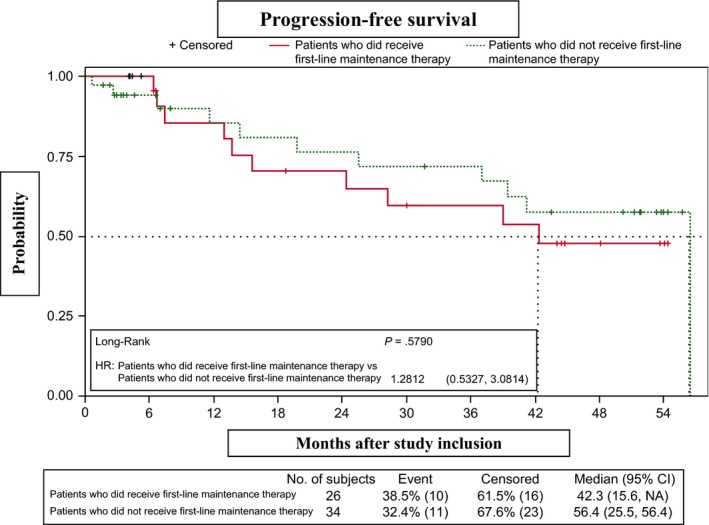
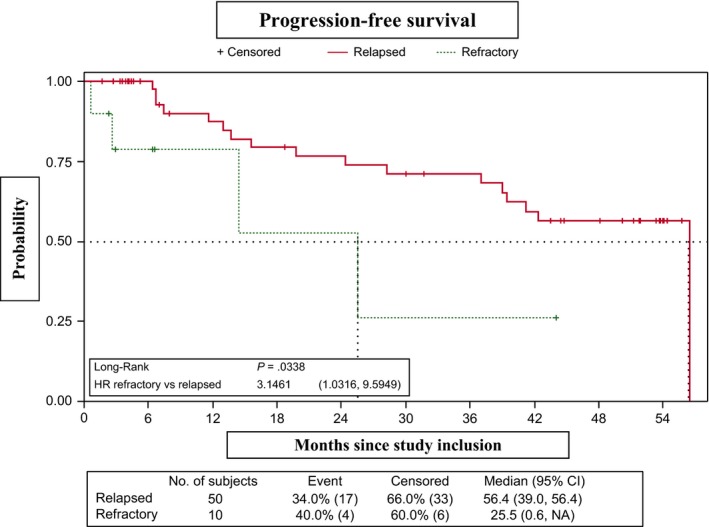
Thirty-three (55%) and 42 (70%) patients achieved complete/unconfirmed complete response after three cycles and on completing induction therapy (4-6 cycles), respectively (final overall response rate, 88.3%). Median progression-free survival was 56.4 months (median follow-up, 28.3 months; 95% CI, 15.6-51.2). Overall survival was not reached. Progression-free survival did not differ between patients who received four vs six cycles (P = .6665), nor between patients who did/did not receive rituximab maintenance after first-line therapy (P = .5790). Median progression-free survival in the 10 refractory patients was 25.5 months (95% CI, 0.6-N/A) and was longer in patients who had shown progression of disease after 24 months of first-line therapy (median, 56.4 months; 95% CI, 19.8-56.4) than in those who showed early progression (median, 42.31 months; 95% CI, 24.41-NA) (P = .4258). Thirty-six (60%) patients had grade 3/4 neutropenia. Grade 3/4 febrile neutropenia and infection were recorded during induction (4/60 [6.7%] and 5/60 [8.3%] patients, respectively) and maintenance (2/43 [4.5%] and 4/43 [9.1%] patients, respectively).
This response-adapted treatment with RBMD followed by rituximab maintenance is an effective and well-tolerated salvage treatment for relapsed/refractory follicular lymphoma following first-line immunochemotherapy.
ClinicalTrials.gov # NCT01133158.
对于一线免疫化疗后复发或耐药的滤泡性淋巴瘤患者,缺乏最佳挽救治疗的共识。
这项 II 期试验评估了利妥昔单抗、苯达莫司汀、米托蒽醌和地塞米松(RBMD)在一线免疫化疗后复发或耐药的滤泡性淋巴瘤患者中适应性治疗的疗效和安全性。60 名患者接受了 3 个治疗周期,根据其反应,接受了另外 1 个(完全/未确认完全缓解)或 3 个(部分缓解)周期。对诱导治疗有反应的患者接受利妥昔单抗维持治疗 2 年。
33 名(55%)和 42 名(70%)患者在 3 个周期和完成诱导治疗(4-6 个周期)后分别达到完全/未确认完全缓解(最终总缓解率,88.3%)。中位无进展生存期为 56.4 个月(中位随访时间,28.3 个月;95%CI,15.6-51.2)。总生存期未达到。无进展生存期在接受 4 个周期与 6 个周期的患者之间无差异(P=0.6665),也在一线治疗后接受/未接受利妥昔单抗维持治疗的患者之间无差异(P=0.5790)。10 名耐药患者的中位无进展生存期为 25.5 个月(95%CI,0.6-N/A),在一线治疗后 24 个月时疾病进展的患者(中位,56.4 个月;95%CI,19.8-56.4)的中位无进展生存期长于早期进展的患者(中位,42.31 个月;95%CI,24.41-N/A)(P=0.4258)。36 名(60%)患者出现 3/4 级中性粒细胞减少症。诱导治疗期间出现 3/4 级发热性中性粒细胞减少症和感染(4/60 [6.7%]和 5/60 [8.3%]患者)和维持治疗期间(2/43 [4.5%]和 4/43 [9.1%]患者)。
这种基于 RBMD 的适应性治疗,继之以利妥昔单抗维持治疗,是一线免疫化疗后复发/难治性滤泡性淋巴瘤的一种有效且耐受性良好的挽救治疗方法。
ClinicalTrials.gov # NCT01133158。