Imam Talha H, Patail Haris, Patail Hassan
Division of Nephrology, Kaiser Permanente, Fontana, CA, USA.
St. George's University School of Medicine, West Indies, Grenada.
Int J Nephrol Renovasc Dis. 2019 Sep 26;12:213-218. doi: 10.2147/IJNRD.S169336. eCollection 2019.
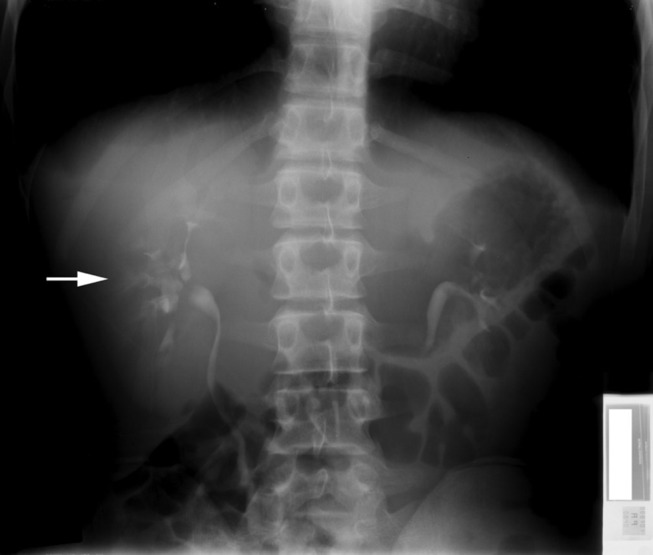
Medullary Sponge Kidney (MSK) disease is a rare congenital malformation of the distal nephron where cystic dilatation is appreciable in the collecting ducts and renal papillae. Most cases of the malformation are thought to arise from a malfunction within neurotrophic factor and tyrosine kinase interactions. Presentation and prognosis are usually indolent; however, they include urinary tract infections (UTI), nephrolithiasis and nephrocalcinosis, distal renal tubular acidosis (dRTA) and hypocitraturia. With an insidious and asymptomatic onset, MSK is a difficult renal manifestation to both diagnose and treat. Difficulty diagnosing MSK today arises from clinical settings deviating from the usage of contrast methods when assessing the urogenital tract. Many healthcare standards for kidney disorders center diagnosis around imaging techniques rather than contrast methods. This ultimately leads to a decrease in the total number of confirmed cases of MSK. Though intra-venous urogram (IVU) remains as the current gold standard to diagnose MSK, other methods such as endoscopy and Multi-detector computed tomography (MDCT) are being put into place. Endoscopic examination and renal biopsy may allow definitive diagnosis; however, such invasive methods may be considered excessive. Moving forward, differential diagnoses for MSK can be made more precisely when patients present with other renal manifestations, especially in groups at risk. These groups include patients between the age of 20 and 30, patients with other renal malformations, high sodium diet patients, hyperparathyroid patients, and patients with family history of MSK. Basic treatment is aimed at controlling stone formation by stabilizing urinary pH. Treatment for patients, especially those prone to forming stones, includes the application of potassium citrate compounds, prophylactic water and diet control, surgical intervention or lithotripsy for removal of symptomatic kidney stones.
髓质海绵肾(MSK)病是一种罕见的远端肾单位先天性畸形,集合管和肾乳头出现明显的囊性扩张。大多数这种畸形病例被认为是由神经营养因子和酪氨酸激酶相互作用的功能障碍引起的。其临床表现和预后通常较为隐匿;然而,包括尿路感染(UTI)、肾结石和肾钙质沉着症、远端肾小管酸中毒(dRTA)和低枸橼酸尿症。由于起病隐匿且无症状,MSK是一种难以诊断和治疗的肾脏表现。如今诊断MSK的困难源于临床评估泌尿生殖道时偏离了造影方法的使用。许多肾脏疾病的医疗标准将诊断集中在成像技术而非造影方法上。这最终导致MSK确诊病例总数减少。尽管静脉肾盂造影(IVU)仍是目前诊断MSK的金标准,但其他方法如内窥镜检查和多排螺旋计算机断层扫描(MDCT)也正在被采用。内窥镜检查和肾活检可能有助于明确诊断;然而,这种侵入性方法可能被认为过度。展望未来,当患者出现其他肾脏表现时,尤其是在高危人群中,可以更精确地进行MSK的鉴别诊断。这些人群包括20至30岁的患者、有其他肾脏畸形的患者、高钠饮食患者、甲状旁腺功能亢进患者以及有MSK家族史的患者。基本治疗旨在通过稳定尿液pH值来控制结石形成。对患者的治疗,尤其是那些容易形成结石的患者,包括应用柠檬酸钾化合物、预防性饮水和饮食控制、手术干预或碎石术以清除有症状的肾结石。