Bertolotti Antoine, Milpied Brigitte, Fouéré Sébastien, Dupin Nicolas, Cabié André, Derancourt Christian
EA 4537, Antilles University, Martinique, France.
Infectious Diseases, Centre Hospitalier Universitaire de la Réunion, Saint-Pierre, La Réunion, France.
Dermatol Ther (Heidelb). 2019 Dec;9(4):761-774. doi: 10.1007/s13555-019-00328-z. Epub 2019 Oct 13.
Several therapeutic options are available to manage anogenital warts (AGWs). However, no hierarchy of treatments is provided in the latest European and American recommendations. This study aimed to determine the efficacy and safety of local treatments for the management of AGWs.
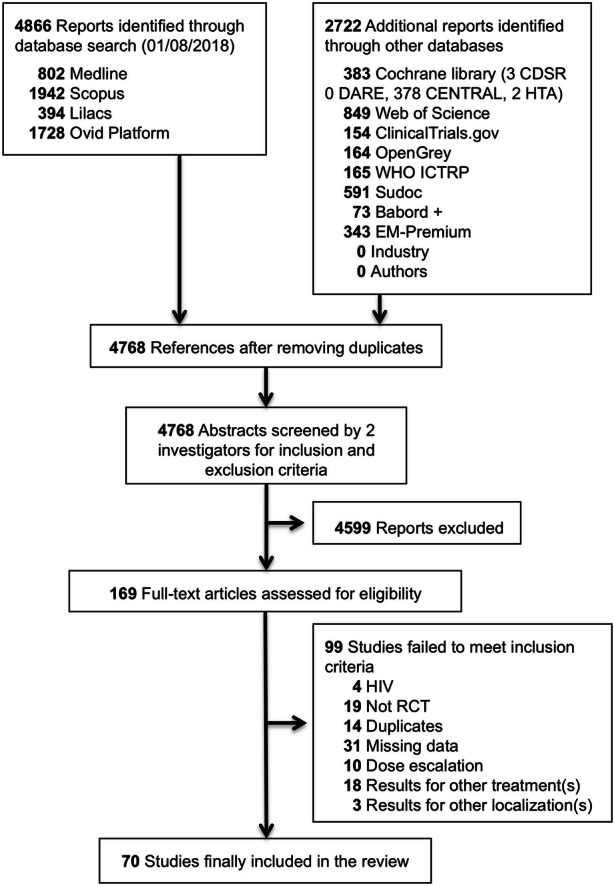
A search was conducted through 12 databases from inception to August 2018. All randomized controlled trials (RCTs) in which at least one parallel treatment group composed of immunocompetent adults with AGWs received at least one provider-administered or patient-administered treatment were included. Risk of bias assessment and meta-analyses of aggregated study data were performed on the basis of the Cochrane Handbook, and quality of evidence evaluation followed the Grading of Recommendation Assessment, Development and Evaluation (GRADE) approach. Primary endpoints were complete clearance and recurrence at 3 months.
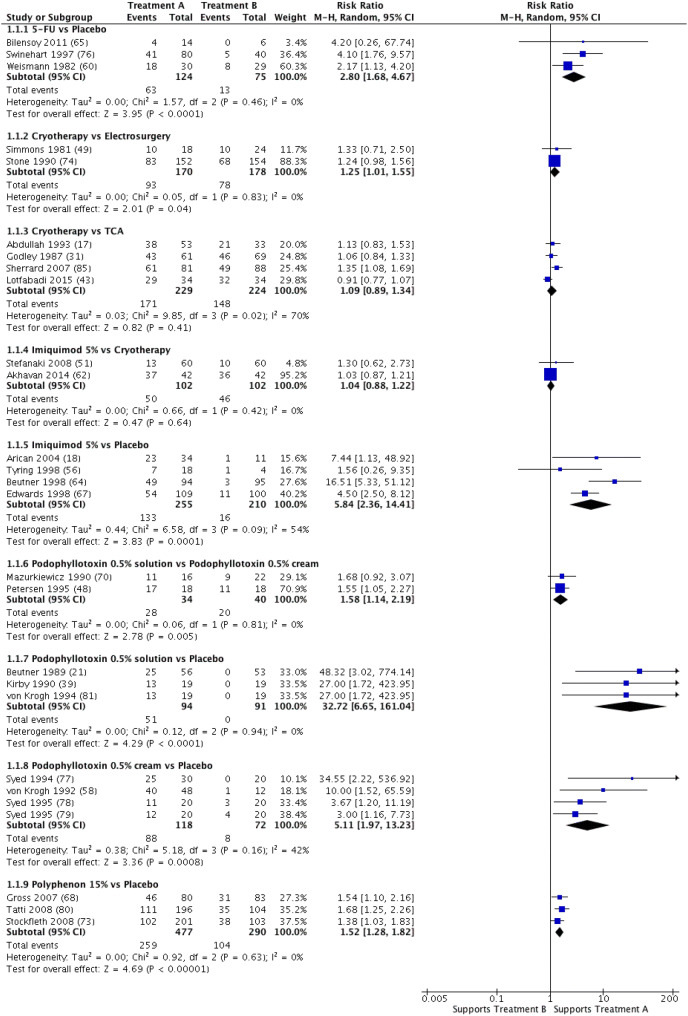
Seventy RCTs (9931 patients) were included. All but four RCTs had a high risk of bias. CO laser was slightly more efficacious than cryotherapy [risk ratio (RR) 2.05; 95% confidence interval (CI) 1.61-2.62], with fewer recurrences at 3 months (RR 0.28; 95% CI 0.09-0.89). Electrosurgery was slightly more efficacious than cryotherapy. No differences in efficacy or side effects were found between cryotherapy and imiquimod or trichloroacetic acid. Podophyllotoxin gel was slightly more efficacious than podophyllotoxin cream. 5-Fluorouracil (5-FU) was slightly more efficacious and caused less erosion than CO laser (RR 1.37; 95% CI 1.11-1.70).
The vast majority of included RCTs had a low level of evidence, thereby preventing the establishment of a hierarchy of treatments. Nevertheless, our results provide an overview of the main AGW treatments available for general practitioners and specialists. While provider-administered treatments are superior, patient-administered treatments (e.g., imiquimod, podophyllotoxin) are useful solutions for compliant patients.
PROSPERO-CRD42015025827.
有多种治疗方法可用于处理肛门生殖器疣(AGW)。然而,最新的欧美指南并未给出治疗方法的优先顺序。本研究旨在确定局部治疗AGW的疗效和安全性。
从数据库建库至2018年8月,通过12个数据库进行检索。纳入所有随机对照试验(RCT),其中至少有一个平行治疗组,由免疫功能正常的成年AGW患者组成,接受至少一种由医护人员实施或患者自行实施的治疗。基于Cochrane手册进行偏倚风险评估和汇总研究数据的荟萃分析,证据质量评估遵循推荐分级评估、制定与评价(GRADE)方法。主要终点为3个月时的完全清除率和复发率。
纳入70项RCT(9931例患者)。除4项RCT外,所有研究均存在高偏倚风险。CO2激光比冷冻疗法稍有效[风险比(RR)2.05;95%置信区间(CI)1.61 - 2.62],3个月时复发较少(RR 0.28;95% CI 0.09 - 0.89)。电外科手术比冷冻疗法稍有效。冷冻疗法与咪喹莫特或三氯乙酸在疗效或副作用方面无差异。鬼臼毒素凝胶比鬼臼毒素乳膏稍有效。5-氟尿嘧啶(5-FU)比CO2激光稍有效且糜烂较少(RR 1.37;95% CI 1.11 - 1.70)。
绝大多数纳入的RCT证据水平较低,因此无法确定治疗方法的优先顺序。尽管如此,我们的结果为全科医生和专科医生提供了主要AGW治疗方法的概述。虽然由医护人员实施的治疗更优,但患者自行实施的治疗(如咪喹莫特、鬼臼毒素)对于依从性好的患者是有用的解决方案。
PROSPERO - CRD42015025827