Zhang Yan-Zhuo, Wang Xue, Wu Jia-Min, Song Chun-Yu, Cui Xiao-Guang
Department of Anesthesiology, China and Heilongjiang Key Laboratory for Anesthesia and Critical Care, The Second Affiliated Hospital of Harbin Medical University, Harbin, China.
Front Pharmacol. 2019 Sep 19;10:1091. doi: 10.3389/fphar.2019.01091. eCollection 2019.
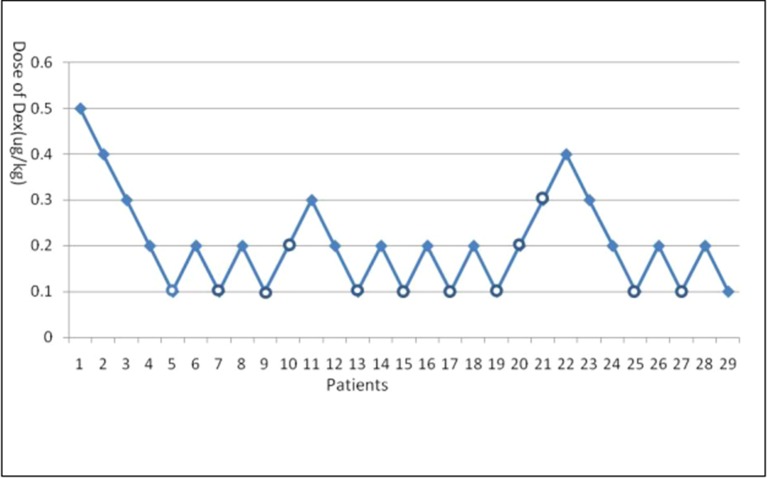
Emergence agitation (EA) is a common pediatric complication after sevoflurane anesthesia that can be prevented with dexmedetomidine. However, an inappropriate dose of dexmedetomidine can cause prolonged sedation and cardiovascular complications. Thus, we evaluated the optimal dose (ED95) of dexmedetomidine for preventing EA with sevoflurane and remifentanil anesthesia after pediatric tonsillectomy and adenoidectomy. We enrolled American Society of Anesthesiologists (ASA) I and II children 3-7 years of age who underwent tonsillectomy with adenoidectomy. During induction, dexmedetomidine was infused for 10 min. Anesthesia was induced with sevoflurane and maintained with sevoflurane and remifentanil, resulting in a bispectral spectrum index (BIS) range from 40 to 60. Extubation time, surgical and anesthetic duration time, and duration time in the postanesthesia care unit (PACU) stay were recorded. EA [measured with Pediatric Anaesthesia Emergence Delirium (PAED) scores] and pain [measured with Face, Legs, Activity, Cry, Consolability (FLACC) scores] were assessed at extubation (E0), 15 min after extubation (E1), and 30 min after extubation (E2). If EA occurred, the next surgical procedure included increased dexmedetomidine by 0.1 μg/kg, and if not, the drug was reduced by 0.1 μg/kg. The 50% effective dose (ED50) of dexmedetomidine for preventing EA after sevoflurane and remifentanil anesthesia for tonsillectomy and adenoidectomy was 0.13 μg/kg, and its 95% confidence interval is 0.09-0.19 μg/kg; ED95 was 0.30 μg/kg, and its 95% confidence interval is 0.21-1.00 μg/kg. Intravenous dexmedetomidine infusion at ED50 (0.13 μg/kg) or ED95 (0.30 μg/kg) during induction for 10 min can prevent half or almost all EA after sevoflurane and remifentanil anesthesia during pediatric tonsillectomy and adenoidectomy.
苏醒期躁动(EA)是七氟醚麻醉后常见的儿科并发症,右美托咪定可预防该并发症。然而,右美托咪定剂量不当会导致镇静时间延长和心血管并发症。因此,我们评估了小儿扁桃体切除术和腺样体切除术后,使用七氟醚和瑞芬太尼麻醉时预防EA的右美托咪定最佳剂量(ED95)。我们纳入了年龄在3至7岁、美国麻醉医师协会(ASA)分级为I级和II级且接受扁桃体切除术和腺样体切除术的儿童。诱导期,右美托咪定输注10分钟。用七氟醚诱导麻醉,并用七氟醚和瑞芬太尼维持麻醉,使脑电双频指数(BIS)维持在40至60之间。记录拔管时间、手术和麻醉持续时间以及在麻醉后恢复室(PACU)停留的持续时间。在拔管时(E0)、拔管后15分钟(E1)和拔管后30分钟(E2)评估EA[用小儿麻醉苏醒期谵妄(PAED)评分衡量]和疼痛[用面部、腿部、活动、哭闹、安慰(FLACC)评分衡量]。如果发生EA,下一次手术中右美托咪定剂量增加0.1μg/kg,如果未发生,则药物剂量减少0.1μg/kg。小儿扁桃体切除术和腺样体切除术中,七氟醚和瑞芬太尼麻醉后预防EA的右美托咪定50%有效剂量(ED50)为0.13μg/kg,其95%置信区间为0.09 - 0.19μg/kg;ED95为0.30μg/kg,其95%置信区间为0.21 - 1.00μg/kg。诱导期静脉输注ED50(0.13μg/kg)或ED95(0.30μg/kg)的右美托咪定10分钟,可预防小儿扁桃体切除术和腺样体切除术中七氟醚和瑞芬太尼麻醉后半数或几乎所有的EA。