School of Public Health & Community Medicine, University of New South Wales (UNSW) Sydney, Kensington NSW, Australia.
National Institute of Public Health, Lot no 80, Street 289, Phnom Penh, Cambodia.
Health Policy Plan. 2019 Oct 1;34(Supplement_1):i4-i13. doi: 10.1093/heapol/czz011.
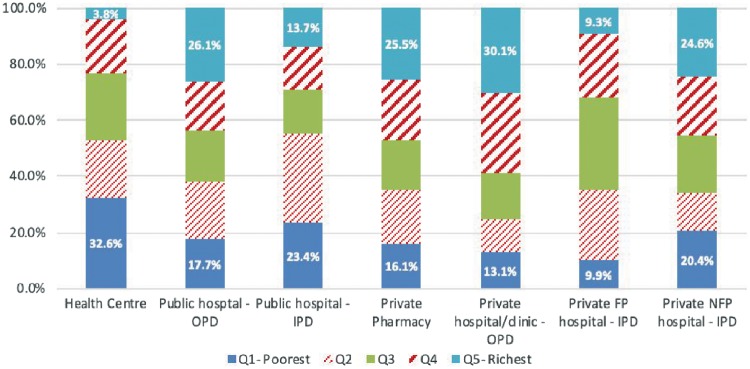
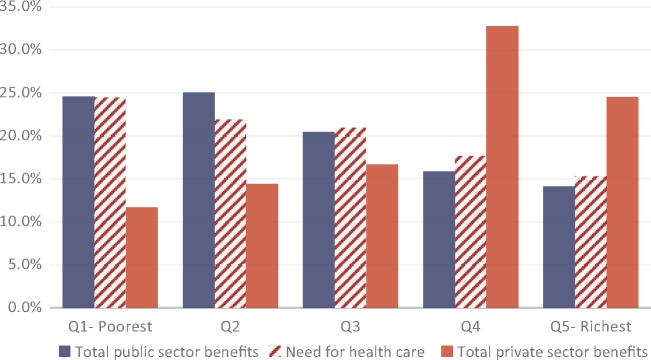
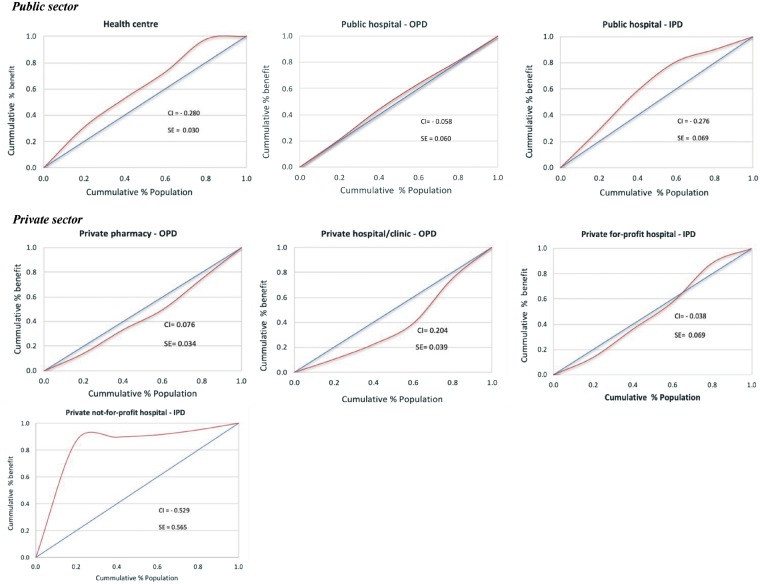
Cambodia's healthcare system has seen significant improvements in the last two decades. Despite this, access to quality care remains problematic, particularly for poor rural Cambodians. The government has committed to universal health coverage (UHC) and is reforming the health financing system to align with this goal. The extent to which the reforms have impacted the poor is not always clear. Using a system-wide approach, this study assesses how benefits from healthcare spending are distributed across socioeconomic groups in Cambodia. Benefit incidence analysis was employed to assess the distribution of benefits from health spending. Primary data on the use of health services and the costs associated with it were collected through a nationally representative cross-sectional survey of 5000 households. Secondary data from the 2012-14 Cambodia National Health Accounts and other official documents were used to estimate the unit costs of services. The results indicate that benefits from health spending at the primary care level in the public sector are distributed in favour of the poor, with about 32% of health centre benefits going to the poorest population quintile. Public hospital outpatient benefits are quite evenly distributed across all wealth quintiles, although the concentration index of -0.058 suggests a moderately pro-poor distribution. Benefits for public hospital inpatient care are substantially pro-poor. The private sector was significantly skewed towards the richest quintile. Relative to health need, the distribution of total benefits in the public sector is pro-poor while the private sector is relatively pro-rich. Looking across the entire health system, health financing in Cambodia appears to benefit the poor more than the rich but a significant proportion of spending remains in the private sector which is largely pro-rich. There is the need for some government regulation of the private sector if Cambodia is to achieve its UHC goals.
柬埔寨的医疗保健系统在过去二十年中取得了重大进展。尽管如此,获得高质量医疗保健的机会仍然存在问题,特别是对于贫困的农村柬埔寨人来说。政府致力于实现全民健康覆盖,并正在改革卫生融资系统,以实现这一目标。改革对贫困人口的影响程度并不总是清楚的。本研究采用系统方法,评估医疗支出的效益在柬埔寨社会经济群体中的分配情况。受益情况分析用于评估卫生支出效益的分配情况。通过对 5000 户家庭进行全国代表性的横断面调查,收集了关于卫生服务使用情况及其相关费用的主要数据。利用 2012-2014 年柬埔寨国家卫生账户和其他官方文件中的二级数据来估计服务的单位成本。结果表明,公共部门初级保健水平的医疗支出效益有利于贫困人口,约有 32%的卫生中心效益流向最贫困的五分位数人群。公立医院门诊效益在所有财富五分位数中分布较为均匀,尽管集中指数为-0.058,表明分配情况略有利于穷人。公立医院住院治疗效益明显有利于穷人。私立部门则明显偏向最富裕的五分位数。相对于卫生需求,公共部门的总效益分配有利于穷人,而私立部门则相对有利于富人。纵观整个卫生系统,柬埔寨的卫生融资似乎使穷人受益多于富人,但仍有相当一部分支出留在私立部门,而私立部门主要有利于富人。如果柬埔寨要实现全民健康覆盖的目标,就需要对私立部门进行一些政府监管。