Takano Masayuki, Sugahara Keisuke, Koyachi Masahide, Odaka Kento, Matsunaga Satoru, Homma Shinya, Abe Shinichi, Katakura Akira, Shibahara Takahiko
1Department of Oral and Maxillofacial Surgery, Tokyo Dental College, 2-9-18 Kandamisaki-cho, Chiyoda-ku, Tokyo, 101-0061 Japan.
2Department of Oral Pathobiological Science and Surgery, Tokyo Dental College, 2-9-18 Kandamisaki-cho, Chiyoda-ku, Tokyo, 101-0061 Japan.
Maxillofac Plast Reconstr Surg. 2019 Oct 17;41(1):43. doi: 10.1186/s40902-019-0228-y. eCollection 2019 Dec.
Reconstructive surgery is often required for tumors of the oral and maxillofacial region, irrespective of whether they are benign or malignant, the area involved, and the tumor size. Recently, three-dimensional (3D) models are increasingly used in reconstructive surgery. However, these models have rarely been adapted for the fabrication of custom-made reconstruction materials. In this report, we present a case of maxillary reconstruction using a laboratory-engineered, custom-made mesh plate from a 3D model.
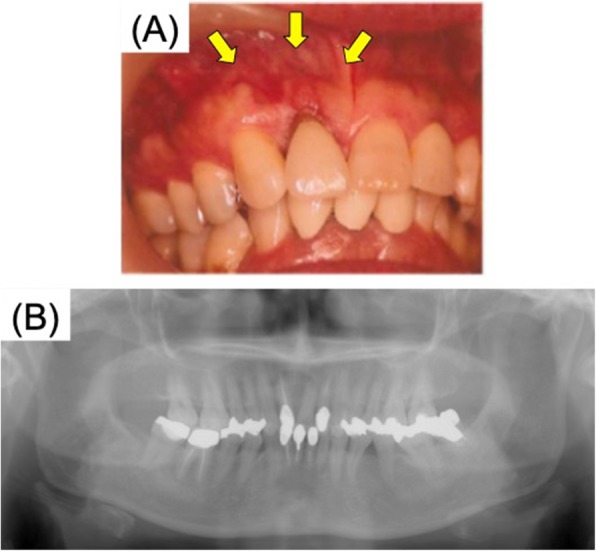
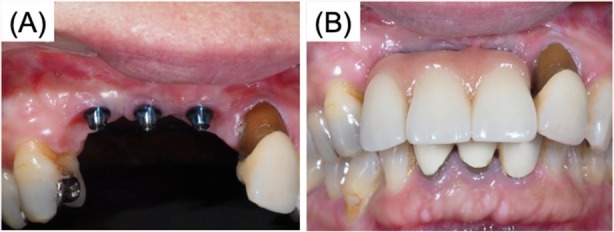
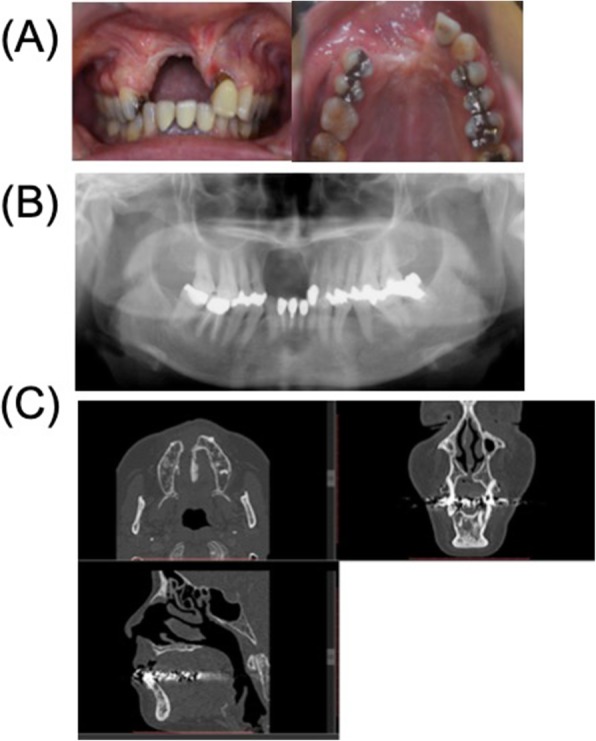
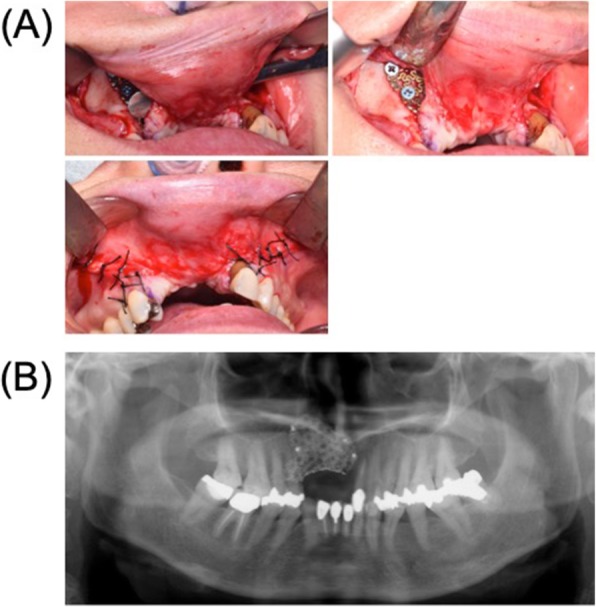
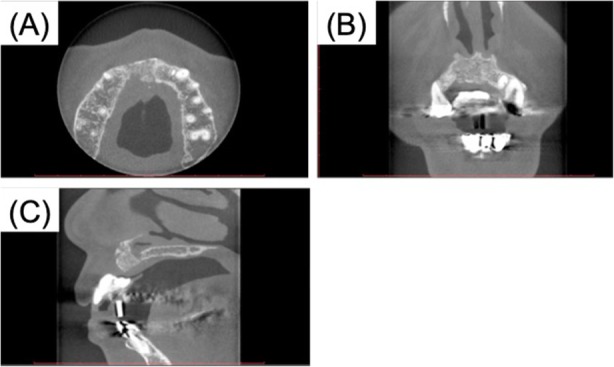
The patient was a 56-year-old female, who had undergone maxillary resection in 2011 for intraoral squamous cell carcinoma that presented as a swelling of the anterior maxillary gingiva. Five years later, there was no recurrence of the malignant tumor and a maxillary reconstruction was planned. Computed tomography (CT) revealed a large bony defect in the dental-alveolar area of the anterior maxilla. Using the CT data, a 3D model of the maxilla was prepared, and the site of reconstruction determined. A custom-made mesh plate was fabricated using the 3D model (Okada Medical Supply, Tokyo, Japan). We performed the reconstruction using the custom-made titanium mesh plate and the particulate cancellous bone and marrow graft from her iliac bone. We employed the tunneling flap technique without alveolar crest incision, to prevent surgical wound dehiscence, mesh exposure, and alveolar bone loss. Ten months later, three dental implants were inserted in the graft. Before the final crown setting, we performed a gingivoplasty with palate mucosal graft. The patient has expressed total satisfaction with both the functional and esthetic outcomes of the procedure.
We have successfully performed a maxillary and dental reconstruction using a custom-made, pre-bent titanium mesh plate.
无论口腔颌面部肿瘤是良性还是恶性,涉及的区域以及肿瘤大小如何,通常都需要进行重建手术。近年来,三维(3D)模型在重建手术中的应用越来越广泛。然而,这些模型很少被用于定制重建材料的制作。在本报告中,我们展示了一例使用基于3D模型在实验室制作的定制网板进行上颌骨重建的病例。
患者为一名56岁女性,2011年因表现为上颌前部牙龈肿胀的口腔鳞状细胞癌接受了上颌骨切除术。五年后,恶性肿瘤未复发,遂计划进行上颌骨重建。计算机断层扫描(CT)显示上颌前部牙槽区域存在大的骨缺损。利用CT数据,制作了上颌骨的3D模型,并确定了重建部位。使用该3D模型制作了定制网板(日本东京冈田医疗用品公司)。我们使用定制的钛网板以及取自患者髂骨的颗粒状松质骨和骨髓移植进行了重建。我们采用了不切开牙槽嵴的隧道皮瓣技术,以防止手术伤口裂开、网板暴露和牙槽骨吸收。十个月后,在移植部位植入了三颗牙种植体。在安装最终牙冠之前,我们进行了腭黏膜移植牙龈成形术。患者对该手术的功能和美学效果均表示完全满意。
我们成功地使用定制的预弯钛网板进行了上颌骨和牙齿重建。