CH de Niort, Service des Maladies Infectieuses et Tropicale, Niort, France.
CHRU de Tours, Unité d'Épidémiologie des données cliniques, EpiDcliC, Tours, France.
PLoS One. 2019 Oct 25;14(10):e0223857. doi: 10.1371/journal.pone.0223857. eCollection 2019.
We assessed the determinants of mortality in infective endocarditis (IE), using the national hospital discharge databases (HDD) in 2011.
IE stays were extracted from the national HDD, with a definition based on IE-related diagnosis codes. This definition has been assessed according to Duke criteria by checking a sample of medical charts of IE giving a predictive positive value of 86.1% (95% confidence interval (CI): 82.7% - 89.5%). The impact of heart valve surgery on survival has been studied if performed during the initial stay, and over the year of follow-up. Risk factors of in-hospital mortality were identified using logistic regression model for the initial stay and Cox Time-dependent model for the 1-year mortality.
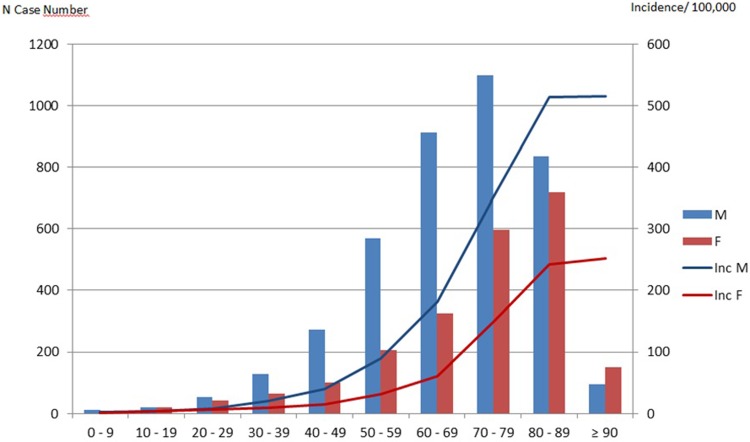
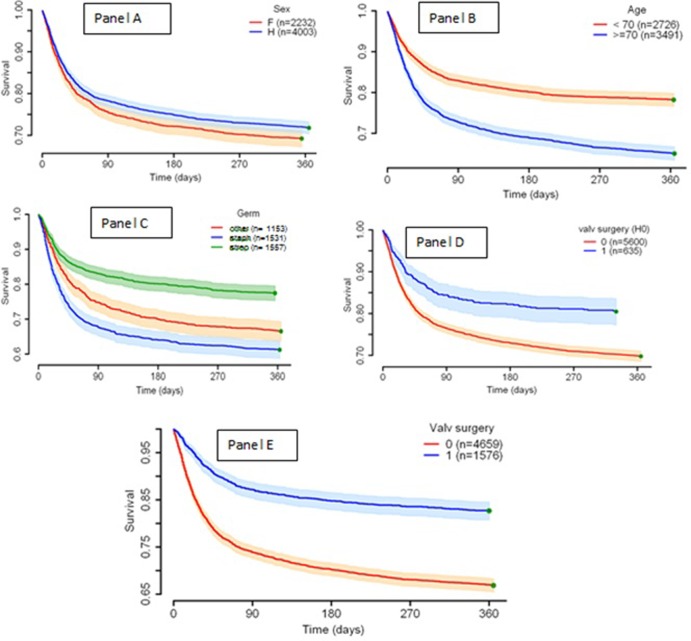
The analysis included 6,235 patients. The annual incidence of definite IEs was 63 cases/million residents. Staphylococci and Streptococci were the most common bacteria (44% and 45%, respectively). A valvular surgery was performed in 20% of cases, but substantial variations existed between hospitals. The in-hospital mortality was 21% (ranging 12% to 27% according to the region of patients), associated with age>70, chronic liver disease, renal failure, S. aureus, P. aeruginosa or candida infection and strokes whereas valvular surgery, a native valve IE or intraveinous drug use (right heart IE) were significantly protective for an initial death. The same factors were associated with the one-year mortality, except for valvular surgery which was associated with a 1.4-fold higher risk of death during the year post IE.
We reported a high IE incidence rate. Valvular surgery was considerably less frequent in this study than in the previous published data (near 50%) whereas mortality was similar. Surgery was associated with higher survival if undergone within the initial stay. There were significant regional differences in frequency of surgery but it did not impact mortality.
我们使用 2011 年全国住院数据库(HDD)评估感染性心内膜炎(IE)的死亡率决定因素。
从全国 HDD 中提取 IE 住院记录,使用基于 IE 相关诊断代码的定义。根据 Duke 标准检查 IE 病历样本对该定义进行了评估,得出预测阳性值为 86.1%(95%置信区间(CI):82.7% - 89.5%)。如果在初始住院期间或随访的 1 年内进行心脏瓣膜手术,研究其对生存率的影响。使用逻辑回归模型确定初始住院期间的住院死亡率的危险因素,并使用 Cox 时间依赖性模型确定 1 年死亡率的危险因素。
分析纳入了 6235 例患者。明确的 IE 年发病率为 63 例/百万居民。葡萄球菌和链球菌是最常见的细菌(分别为 44%和 45%)。20%的病例进行了瓣膜手术,但医院之间存在很大差异。住院死亡率为 21%(根据患者所在地区,范围为 12%至 27%),与年龄>70 岁、慢性肝病、肾衰竭、金黄色葡萄球菌、铜绿假单胞菌或念珠菌感染和中风相关,而瓣膜手术、原发性瓣膜 IE 或静脉内药物使用(右心 IE)则显著降低初始死亡风险。同样的因素与 1 年死亡率相关,除了瓣膜手术与 IE 后 1 年内死亡风险增加 1.4 倍相关。
我们报告了一个较高的 IE 发病率。在本研究中,瓣膜手术明显低于之前发表的数据(接近 50%),而死亡率相似。如果在初始住院期间进行手术,则与生存率提高相关。手术频率存在明显的地区差异,但并未影响死亡率。