Roy Ashok, Stanford Sophia, Nunn Sean, Alves Sue, Sargant Nigel, Rangarajan Savita, Smith Emily Arbuthnot, Bell John, Dayal Sanjeev, Cecil Tom, Tzivanakis Alexios, Kruzhkova Irina, Solomon Cristina, Knaub Sigurd, Moran Brendan, Mohamed Faheez
Basingstoke and North Hampshire Hospital, Basingstoke, UK.
University Hospital Southampton NHS Foundation Trust, UK.
J Thromb Haemost. 2020 Feb;18(2):352-363. doi: 10.1111/jth.14665. Epub 2019 Nov 26.
Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy for pseudomyxoma peritonei (PMP) is associated with excessive bleeding and acquired fibrinogen deficiency. Maintaining plasma fibrinogen may support hemostasis.
To compare hemostatic efficacy and safety of human fibrinogen concentrate (HFC) vs cryoprecipitate as fibrinogen sources for bleeding patients with acquired fibrinogen deficiency undergoing PMP CRS.
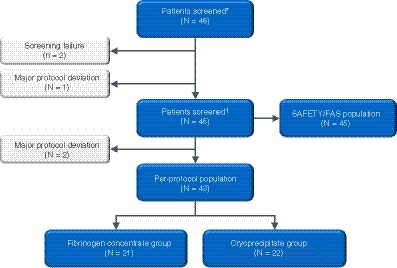
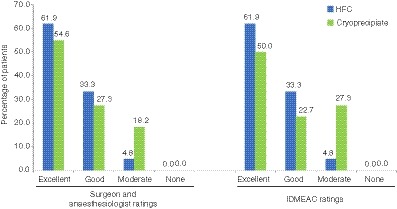
FORMA-05 was an off-label single-center, prospective, randomized, controlled phase 2 study. Patients undergoing PMP surgery with predicted intraoperative blood loss ≥2 L received human fibrinogen concentrate (HFC; 4 g) or cryoprecipitate (two pools of 5 units, containing approximately 4.0-4.6 g fibrinogen), repeated as needed. The primary endpoint was a composite of intraoperative and postoperative efficacy, graded using objective 4-point scales and adjudicated by an independent committee.
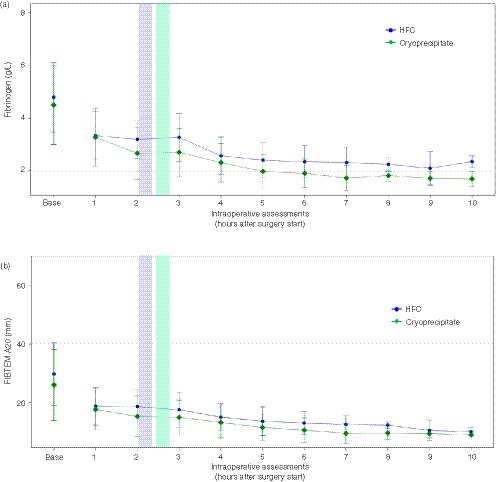
One hundred percent of patients receiving HFC (95% confidence interval: 83.9-100.0, n = 21) or cryoprecipitate (84.6-100.0, n = 22) achieved hemostatic success. HFC demonstrated noninferior efficacy (P = .0095; post hoc) and arrived in the operating room 46 minutes faster. There were significantly greater mean increases with HFC vs cryoprecipitate in plasma fibrinogen (0.78 vs 0.35 g/L; P < .0001) and FIBTEM A20 (3.33 vs 0.93 mm; P = .003). Factor XIII, factor VIII, and von Willebrand factor activity were maintained throughout surgery. Only red blood cells were transfused intraoperatively (median units: HFC group, 1.0; cryoprecipitate group, 0.5). Thromboembolic events were detected with cryoprecipitate only. Safety was otherwise comparable between groups.
Human fibrinogen concentrate was hemostatically efficacious in patients undergoing major abdominal PMP surgery, with a favorable safety profile. These results are relevant to other surgical settings where bleeding and acquired fibrinogen deficiency occur.
腹膜假黏液瘤(PMP)的细胞减灭术(CRS)联合腹腔内热灌注化疗与出血过多及获得性纤维蛋白原缺乏有关。维持血浆纤维蛋白原水平可能有助于止血。
比较人纤维蛋白原浓缩物(HFC)与冷沉淀作为纤维蛋白原来源,对接受PMP CRS且有获得性纤维蛋白原缺乏的出血患者的止血效果和安全性。
FORMA-05是一项单中心、前瞻性、随机、对照的2期非适应证研究。预计术中失血≥2L的接受PMP手术的患者接受人纤维蛋白原浓缩物(HFC;4g)或冷沉淀(两袋,每袋5单位,含约4.0 - 4.6g纤维蛋白原),根据需要重复使用。主要终点是术中及术后疗效的综合指标,采用客观的4分制量表进行分级,并由独立委员会判定。
接受HFC的患者(95%置信区间:83.9 - 100.0,n = 21)和接受冷沉淀的患者(84.6 - 100.0,n = 22)100%实现止血成功。HFC显示出非劣效性疗效(P = 0.0095;事后分析),且比冷沉淀提前46分钟送达手术室。与冷沉淀相比,HFC使血浆纤维蛋白原平均增加幅度显著更大(0.78 vs 0.35g/L;P < 0.0001),FIBTEM A20也更大(3.33 vs 0.93mm;P = 0.003)。整个手术过程中因子 XIII、因子 VIII 和血管性血友病因子活性均得以维持。术中仅输注了红细胞(中位数单位:HFC组为1.0;冷沉淀组为0.5)。仅在冷沉淀组检测到血栓栓塞事件。两组在其他方面的安全性相当。
人纤维蛋白原浓缩物对接受大型腹部PMP手术的患者止血有效,且安全性良好。这些结果与其他发生出血和获得性纤维蛋白原缺乏的手术情况相关。