Chipollini Juan, da Costa Walter Henriques, Werneck da Cunha Isabela, de Almeida E Paula Felipe, Guilherme O Salles Paulo, Azizi Mounsif, Spiess Philippe E, Abreu Diego, Zequi Stênio de Cássio
Department of Surgery, The University of Arizona College of Medicine, 1501 North Campbell Avenue, PO Box 245077, Tucson AZ 85724-5077, USA.
Division of Urology, AC Camargo Cancer Center, São Paulo, Brazil.
Ther Adv Urol. 2019 Oct 13;11:1756287219882600. doi: 10.1177/1756287219882600. eCollection 2019 Jan-Dec.
We aimed to evaluate the prognostic role of programmed-death receptor ligand (PD-L1) in a multinational cohort of patients with localized renal cell carcinoma (RCC).
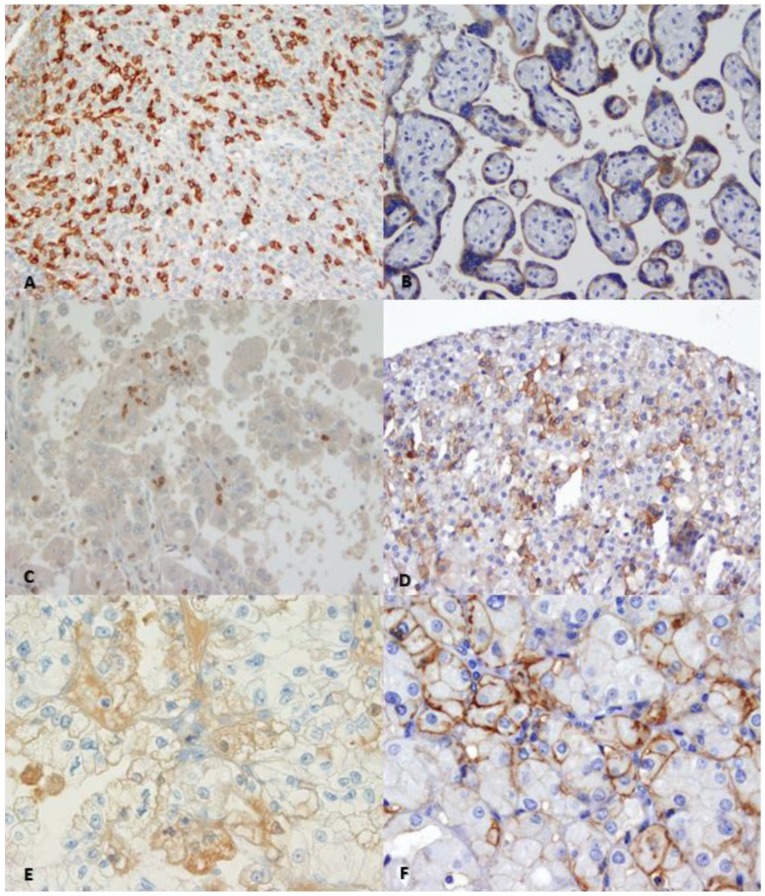
Formalin-fixed paraffin-embedded blocks of 1017 patients from the Latin American Renal Cancer Group were analyzed. Tissue microarrays were immunostained for PD-L1 using a commercially available monoclonal antibody. Expression of PD-L1 in ⩾5% tumor cells was considered positive. PD-1 expression in immune cells was also assessed. All cases were reviewed twice based on antibody expression and compared with a positive control. Cox proportional hazard regression models were used to identify predictors of recurrence-free survival (RFS) and overall survival (OS).
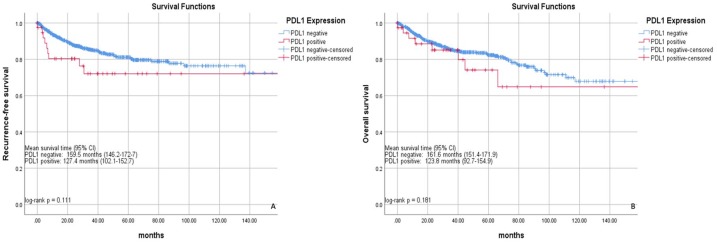
A total of 738 cases with complete follow up met criteria. Median age was 57 [interquartile range (IQR): 49-64] years, and median follow up was 34 (IQR: 15-62.9) months. Median tumor size was 5 cm (IQR: 3.0-7.5 cm). Approximately 8.2% and 7.6% of tumors were PD-L1 and programmed cell-death 1 (PD-1) positive, respectively. PD-L1 and PD-1 positivity were significantly associated with higher tumor stage (both < 0.001), and presence of tumor necrosis and lymphovascular multivariable analyses; PD-L1 positivity was found as a predictor of worse RFS [hazard ratio (HR) = 2.08, = 0.05] and OS (HR = 2.61, = 0.02).
PD-L1 positivity was significantly associated with worse outcomes for patients with localized RCC at intermediate follow up. This marker may help stratify patients for stricter surveillance after surgical treatment and provide a basis for checkpoint-inhibitor therapy in the adjuvant setting.
我们旨在评估程序性死亡受体配体(PD-L1)在多国局部肾细胞癌(RCC)患者队列中的预后作用。
对拉丁美洲肾癌组1017例患者的福尔马林固定石蜡包埋块进行分析。使用市售单克隆抗体对组织微阵列进行PD-L1免疫染色。肿瘤细胞中PD-L1表达≥5%被视为阳性。还评估了免疫细胞中PD-1的表达。所有病例根据抗体表达进行两次复查,并与阳性对照进行比较。使用Cox比例风险回归模型确定无复发生存期(RFS)和总生存期(OS)的预测因素。
共有738例具有完整随访的病例符合标准。中位年龄为57岁[四分位间距(IQR):49 - 64岁],中位随访时间为34(IQR:15 - 62.9)个月。中位肿瘤大小为5 cm(IQR:3.0 - 7.5 cm)。分别约8.2%和7.6%的肿瘤为PD-L1和程序性细胞死亡1(PD-1)阳性。PD-L1和PD-1阳性与更高的肿瘤分期显著相关(均P < 0.001),且与肿瘤坏死和脉管浸润的存在相关;多变量分析显示,PD-L1阳性是RFS较差[风险比(HR) = 2.08,P = 0.05]和OS较差(HR = 2.61,P = 0.02)的预测因素。
在中期随访中,PD-L1阳性与局部RCC患者的较差预后显著相关。该标志物可能有助于对患者进行分层以便在手术治疗后进行更严格的监测,并为辅助治疗中检查点抑制剂治疗提供依据。