Department of Anesthesiology & Critical Care, Mechi Zonal Hospital, Bhadrapur, Nepal.
Department of Anesthesiology & Critical Care Medicine, BP Koirala Institute of Health Sciences, BPKIHS, Dharan, Nepal.
BMC Anesthesiol. 2019 Nov 4;19(1):198. doi: 10.1186/s12871-019-0874-8.
As a part of multimodal analgesia for laparoscopic cholecystectomy, both intraoperative lidocaine and esmolol facilitate postoperative analgesia. Our objective was to compare these two emerging strategies that challenge the use of intraoperative opioids. We aimed to assess if intraoperative esmolol infusion is not inferior to lidocaine infusion for opioid consumption after laparoscopic cholecystectomy.
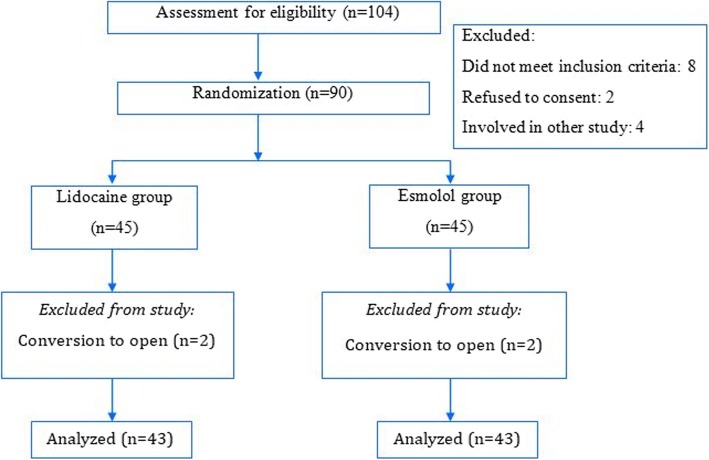
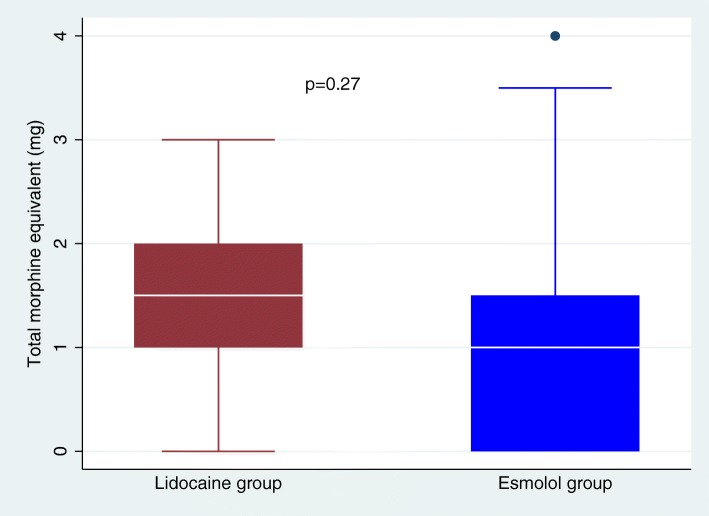
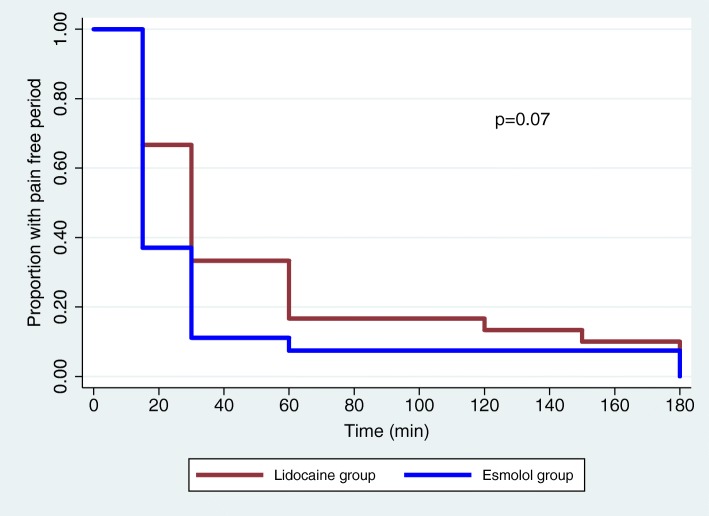
In this prospective, randomized, double-blind, non-inferiority clinical trial, 90 female patients scheduled for elective laparoscopic cholecystectomy received either intravenous (IV) lidocaine bolus 1.5 mg/kg at induction followed by an infusion (1.5 mg/ kg/h) or IV bolus of esmolol 0.5 mg/kg at induction followed by an infusion (5-15 μg/kg/min) till the end of surgery. Remaining aspect of anesthesia followed a standard protocol apart from no intraoperative opioid supplementation. Postoperatively, patients received either morphine or tramadol IV to maintain visual analogue scale (VAS) scores ≤3. The primary outcome was opioid consumption (in morphine equivalents) during the first 24 postoperative hours. Pain and sedation scores, time to first perception of pain and void, and occurrence of nausea/vomiting were secondary outcomes measured up to 24 h postoperatively.
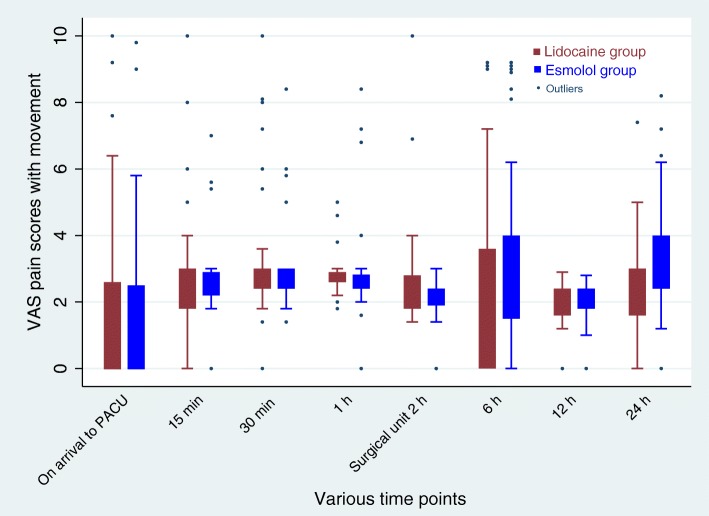
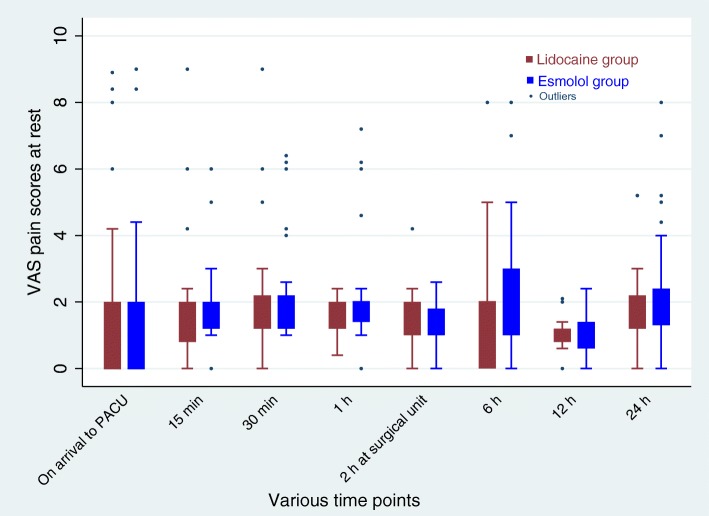
Two patients in each group were excluded from the analysis. The postoperative median (IQR) morphine equivalent consumption in patients receiving esmolol was 1 (0-1.5) mg compared to 1.5 (1-2) mg in lidocaine group (p = 0.27). The median pain scores at various time points were similar between the two groups (p > 0.05). More patients receiving lidocaine were sedated in the post-anesthesia care unit (PACU) than those receiving esmolol (p < 0.05); however, no difference was detected later.
Infusion of esmolol is not inferior to lidocaine in terms of opioid requirement and pain severity in the first 24 h after surgery. Patients receiving lidocaine were more sedated during their stay in PACU than those receiving esmolol.
ClinicalTrials.gov - NCT02327923. Date of registration: December 31, 2014.
作为腹腔镜胆囊切除术多模式镇痛的一部分,术中利多卡因和艾司洛尔都有助于术后镇痛。我们的目的是比较这两种新的策略,挑战术中使用阿片类药物。我们旨在评估术中艾司洛尔输注是否不比利多卡因输注更能减少腹腔镜胆囊切除术后的阿片类药物消耗。
在这项前瞻性、随机、双盲、非劣效性临床试验中,90 名择期行腹腔镜胆囊切除术的女性患者接受静脉注射(IV)利多卡因 1.5mg/kg 诱导,继以输注(1.5mg/kg/h)或 IV 艾司洛尔 0.5mg/kg 诱导,继以输注(5-15μg/kg/min)直至手术结束。除不术中给予阿片类药物补充外,其余麻醉方面遵循标准方案。术后,患者接受吗啡或曲马多静脉注射以维持视觉模拟评分(VAS)≤3。主要结局是术后 24 小时内的阿片类药物消耗(以吗啡等效物计)。疼痛和镇静评分、首次感知疼痛和排尿时间以及恶心/呕吐的发生是术后 24 小时内测量的次要结局。
每组各有 2 例患者被排除在分析之外。接受艾司洛尔的患者术后中位数(IQR)吗啡等效物消耗量为 1(0-1.5)mg,而接受利多卡因的患者为 1.5(1-2)mg(p=0.27)。两组各时间点的中位数疼痛评分相似(p>0.05)。接受利多卡因的患者在麻醉后恢复室(PACU)的镇静程度高于接受艾司洛尔的患者(p<0.05);然而,后来没有发现差异。
在术后 24 小时内,艾司洛尔输注在阿片类药物需求和疼痛严重程度方面并不劣于利多卡因。在 PACU 停留期间,接受利多卡因的患者比接受艾司洛尔的患者镇静程度更高。
ClinicalTrials.gov - NCT02327923。注册日期:2014 年 12 月 31 日。