Kim Dong Hwan, Cho Won Ho, Hur Beong Ik, Cha Seung Heon, Lee Sang Weon, Choi Chang Hwa
Department of Neurosurgery & Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea.
Department of Neurosurgery, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
Brain Tumor Res Treat. 2019 Oct;7(2):132-136. doi: 10.14791/btrt.2019.7.e31.
Gamma knife radiosurgery (GKRS) has become a major alternative in the neurosurgical field. However, many patients complained of considerable discomfort during the fixation of rigid headframe. This study investigated whether our modified procedure could reduce fixation-related pain.
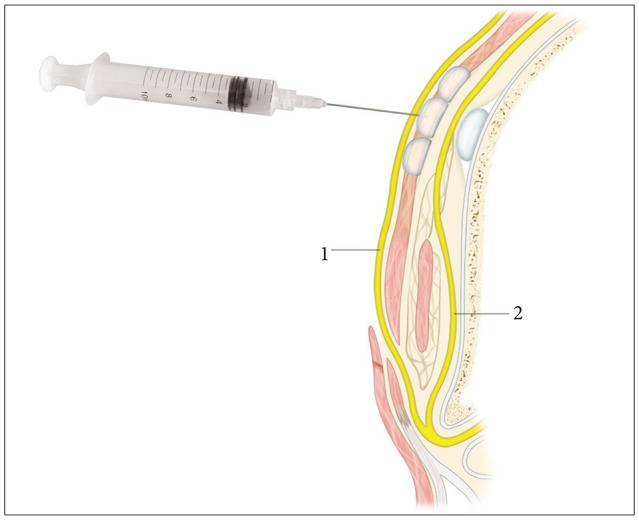
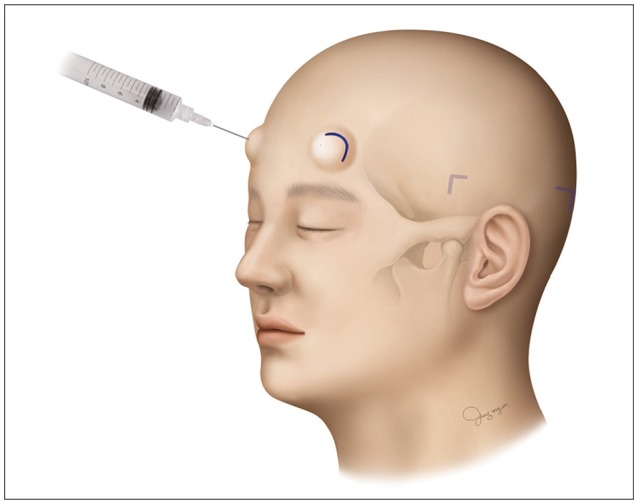
Sixty-six patients who underwent GKRS were enrolled in this study. Thirty-one patients (Group A) underwent the conventional subcutaneous infiltration technique, and 35 patients (Group B) did the modified procedure. In group A, the headframe was held in position by an assistant, and local anesthetics were injected subcutaneously using a 23-gauge spinal needle at pinning sites. Subsequently, pins were applied according to measurements based on spinal needle depth. In group B, with the frame held in position by an assistant, pin sites were marked with a surgical pen under the guidance of needle cap placed on the pin holes. The head frame was then removed, and local anesthetics were injected subcutaneously and periosteally at each marked pin site using a 26-gauge needle. The headframe was then repositioned 5 minutes after local infiltration, and pins were applied according to measurements based on spinal needle depth. To evaluate pain severity during procedures, visual analogue scale (VAS) scores were recorded during local infiltration and frame placement with pins. The pain scores of the two groups were analyzed statistically.
Group B had a significantly lower VAS score during frame placement than group A (7.26 vs. 3.61; <0.001), and mean VAS score at local infiltration was also significantly lower in group B (4.74 vs. 3.74; =0.008).
Patients in group B experienced significantly less pain than those in group A during pin placement. Pre-fixation time advanced local anesthesia might reduce pain during stereotactic procedures, and the use of a 26-gauge needle appeared in less pain during local infiltration.
伽玛刀放射外科手术(GKRS)已成为神经外科领域的一种主要替代方法。然而,许多患者在刚性头架固定过程中抱怨有相当大的不适。本研究调查了我们改良的操作方法是否能减轻与固定相关的疼痛。
66例行GKRS的患者纳入本研究。31例患者(A组)采用传统的皮下浸润技术,35例患者(B组)采用改良操作方法。A组中,助手将头架固定到位,使用23号脊椎穿刺针在固定点皮下注射局部麻醉剂。随后,根据基于脊椎穿刺针深度的测量结果应用固定针。B组中,助手固定头架,在置于针孔上的针帽引导下,用手术笔标记固定点。然后取下头架,使用26号针在每个标记的固定点皮下和骨膜下注射局部麻醉剂。局部浸润5分钟后重新放置头架,根据基于脊椎穿刺针深度的测量结果应用固定针。为了评估操作过程中的疼痛严重程度,在局部浸润和用固定针放置头架时记录视觉模拟量表(VAS)评分。对两组的疼痛评分进行统计学分析。
B组在放置头架时的VAS评分显著低于A组(7.26对3.61;<0.001),B组在局部浸润时的平均VAS评分也显著更低(4.74对3.74;=0.008)。
B组患者在放置固定针时的疼痛明显低于A组患者。预固定时间提前进行局部麻醉可能会减轻立体定向手术过程中的疼痛,并且使用26号针在局部浸润时疼痛较轻。