Cambridge Institute of Public Health, School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom.
Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, Verona, Italy.
PLoS One. 2019 Nov 7;14(11):e0224724. doi: 10.1371/journal.pone.0224724. eCollection 2019.
For a decade, experts have suggested integrating mental health care into primary care to help bridge mental health Treatment Gap. General Practitioners (GPs) are the first port-of-call for many patients with mental ill-health. In Indonesia, the WHO mhGAP is being systematically introduced to its network of 10,000 primary care clinics as an add-on mental health training for pairs of GPs and Nurses, since the end of 2015. In one of 34 provinces, there exists an integrated care model: the co-location of clinical psychologists in primary care clinics. This trial evaluates patient outcomes among those provided mental health care by GPs with those treated by clinical psychologists in primary care.
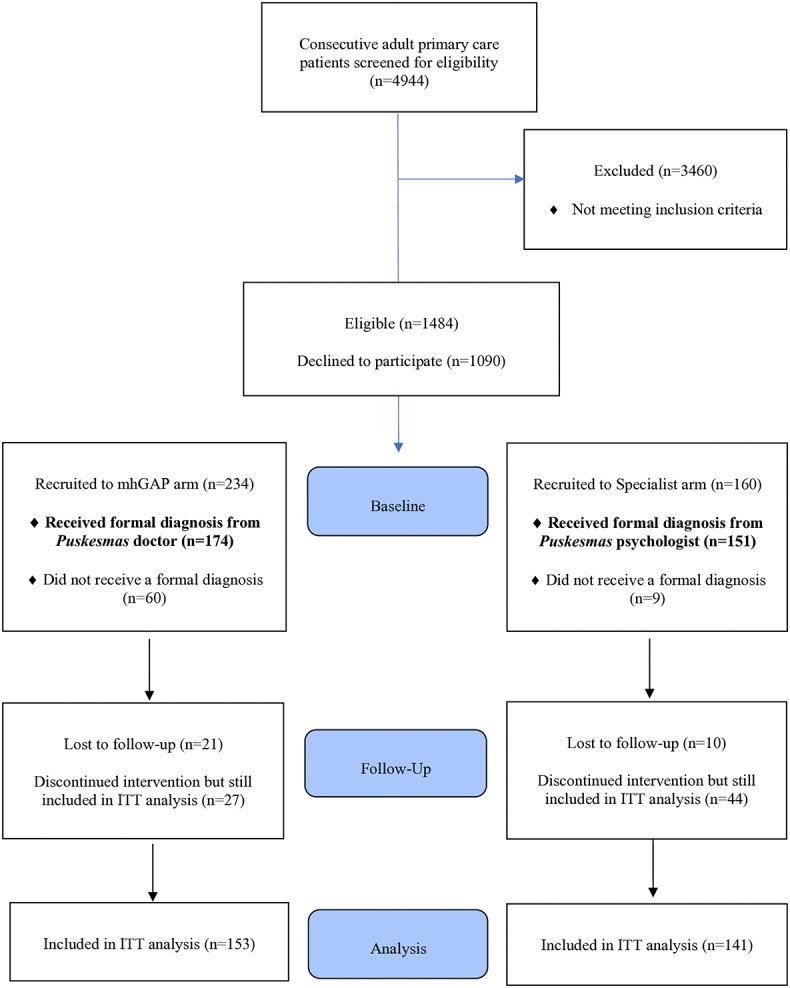
In this partially-randomised, pragmatic, two-arm cluster non-inferiority trial, 14 primary care clinics were assigned to receive the WHO mhGAP training and 14 clinics with the co-location framework were assigned to the Specialist arm. Participants (patients) were blinded to the existence of the other pathway, and outcome assessors were blinded to group assignment. All adult primary care patients who screened positive for psychiatric morbidity were eligible. GPs offered psychosocial and/or pharmacological interventions and Clinical Psychologists offered psychosocial interventions. The primary outcome was health and social functioning as measured by the HoNOS and secondary outcomes include disability measured by WHODAS 2.0, health-related quality of life measured by EQ-5D-3L, and resource use and costs evaluated from a health services perspective, at six months.
153 patients completed the outcome assessment following GP care alongside 141 patients following Clinical Psychologists care. Outcomes of GP care were proven to be statistically not inferior to Clinical Psychologists in reducing symptoms of social and physical impairment, reducing disability, and improving health-related quality of life at six months. Economic analyses indicate lower costs and better outcomes in the Specialist arm and suggest a 50% probability of WHO mhGAP framework being cost-effective at the Indonesian willingness to pay threshold per QALY.
General Practitioners supported by nurses in primary care clinics could effectively manage mild to moderate mental health issues commonly found among primary care patients. They provide non-stigmatising mental health care within community context, helping to reduce the mental health Treatment Gap.
ClinicalTrials.gov NCT02700490.
十年来,专家们一直建议将心理健康护理纳入初级保健,以帮助缩小心理健康治疗差距。全科医生(GP)是许多精神健康不佳患者的首选。自 2015 年底以来,印度尼西亚一直在其 10,000 家初级保健诊所网络中系统地引入世界卫生组织 mhGAP,作为对 GP 和护士的附加心理健康培训。在 34 个省中的一个省,存在一种综合护理模式:临床心理学家在初级保健诊所的共同定位。这项试验评估了由 GP 提供心理健康护理的患者和在初级保健中由临床心理学家治疗的患者的患者结局。
在这项部分随机、实用、双臂非劣效性试验中,将 14 家初级保健诊所分配接受世界卫生组织 mhGAP 培训,将 14 家具有共同定位框架的诊所分配到专科组。参与者(患者)对另一种途径的存在一无所知,结果评估者对分组一无所知。所有筛查出精神疾病的成年初级保健患者均符合条件。GP 提供心理社会和/或药物干预,临床心理学家提供心理社会干预。主要结局是由 HoNOS 测量的健康和社会功能,次要结局包括由 WHODAS 2.0 测量的残疾、由 EQ-5D-3L 测量的健康相关生活质量以及从卫生服务角度评估的资源使用和成本,均在六个月时进行。
在 GP 护理后,有 153 名患者完成了结局评估,在临床心理学家护理后,有 141 名患者完成了评估。GP 护理的结果在六个月时在减轻社会和身体损伤症状、减少残疾和改善健康相关生活质量方面被证明在统计学上不劣于临床心理学家。经济分析表明,在专科组中成本更低,结果更好,并表明在印度尼西亚每 QALY 的意愿支付阈值下,世界卫生组织 mhGAP 框架有 50%的可能性具有成本效益。
在初级保健诊所中由护士支持的全科医生可以有效地管理初级保健患者中常见的轻度至中度心理健康问题。他们在社区环境中提供非污名化的心理健康护理,有助于缩小心理健康治疗差距。
ClinicalTrials.gov NCT02700490。