Scurt Florian G, Menne Jan, Brandt Sabine, Bernhardt Anja, Mertens Peter R, Haller Hermann, Chatzikyrkou Christos
Clinic of Nephrology, Hypertension, Diabetes and Endocrinology, Health Campus Immunology, Infectiology, and Inflammation, Otto-von-Guericke University, Magdeburg, Germany.
Nephrology Section, Hanover Medical School, Hanover, Germany.
Kidney Int Rep. 2019 Jun 21;4(10):1373-1386. doi: 10.1016/j.ekir.2019.06.005. eCollection 2019 Oct.
The aim of the case-control study was to investigate if serum biomarkers indicative of vascular inflammation and endothelial dysfunction can predict the development of microalbuminuria in patients with diabetes mellitus type 2.
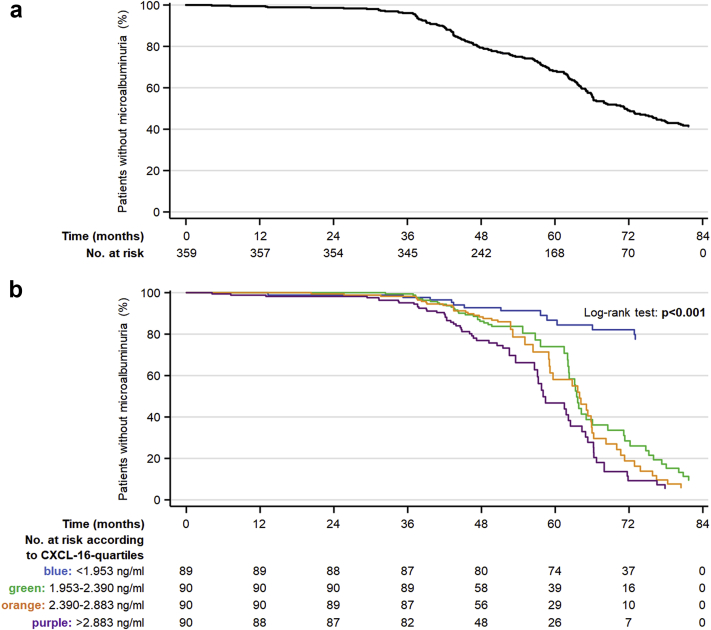
Among participants enrolled in the ROADMAP (Randomized Olmesartan And Diabetes MicroAlbuminuria Prevention) and observational follow-up (OFU) studies, a panel of 15 serum biomarkers was quantified from samples obtained at initiation of the study and tested for associations with the development of new-onset microalbuminuria during follow-up. A case-control study was conducted with inclusion of 172 patients with microalbuminuria and 188 matched controls. Nonparametric inferential, nonlinear regression, mediation, and bootstrapping statistical methods were used for the analysis.
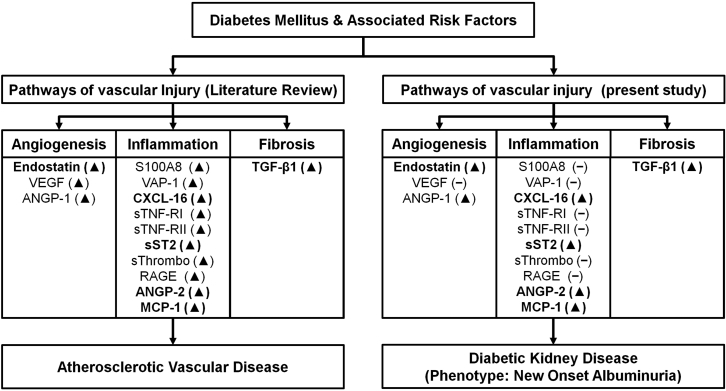
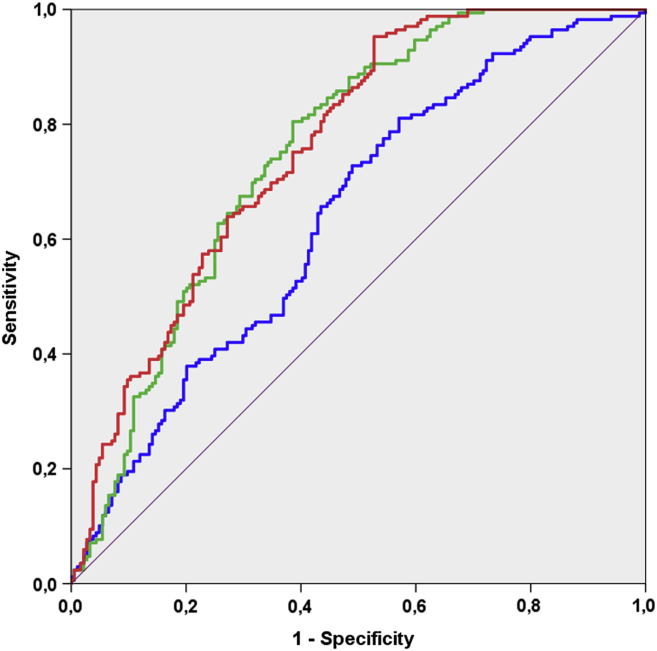
The median follow-up time was 37 months. At baseline, mean concentrations of C-X-C motif chemokine ligand 16 (CXCL-16), transforming growth factor (TGF)-β1 and angiopoietin-2 were higher in patients with subsequent microalbuminuria. In the multivariate analysis, after adjustment for age, sex, body mass index, glycated hemoglobin, duration of diabetes, low-density lipoprotein (LDL), smoking status, blood pressure, baseline urine albumin-to-creatinine ratio (UACR), estimated glomerular filtration rate (eGFR), time of follow-up and cardiovascular disease, CXCL-16 (odds ratio [OR] 2.60, 95% confidence interval [CI] 1.71-3.96), angiopoietin-2 (OR 1.50, 95% CI 1.14-1.98) and TGF-β1 (OR 1.03, 95% CI 1.01-1.04) remained significant predictors of new-onset microalbuminuria ( < 0.001). Inclusion of these biomarkers in conventional clinical risk models for prediction of microalbuminuria increased the area under the curve (AUC) from 0.638 to 0.760 ( < 0.001).
In patients with type 2 diabetes, elevated plasma levels of CXCL-16, angiopoietin-2, and TGF-β1 are independently predictive of microalbuminuria. Thus, these serum markers improve renal risk models beyond established clinical risk factors.
本病例对照研究的目的是调查指示血管炎症和内皮功能障碍的血清生物标志物是否能够预测2型糖尿病患者微量白蛋白尿的发生。
在参与ROADMAP(随机奥美沙坦与糖尿病微量白蛋白尿预防)和观察性随访(OFU)研究的参与者中,从研究开始时采集的样本中对一组15种血清生物标志物进行定量,并检测其与随访期间新发微量白蛋白尿发生的相关性。进行了一项病例对照研究,纳入了172例微量白蛋白尿患者和188例匹配对照。采用非参数推断、非线性回归、中介和自抽样统计方法进行分析。
中位随访时间为37个月。在基线时,随后发生微量白蛋白尿的患者中,C-X-C基序趋化因子配体16(CXCL-16)、转化生长因子(TGF)-β1和血管生成素-2的平均浓度较高。在多变量分析中,在调整年龄、性别、体重指数、糖化血红蛋白、糖尿病病程、低密度脂蛋白(LDL)、吸烟状况、血压、基线尿白蛋白与肌酐比值(UACR)、估计肾小球滤过率(eGFR)、随访时间和心血管疾病后,CXCL-16(比值比[OR]2.60,95%置信区间[CI]1.71-3.96)、血管生成素-2(OR 1.50,95%CI 1.14-1.98)和TGF-β1(OR 1.03,95%CI 1.01-1.04)仍然是新发微量白蛋白尿的显著预测因子(<0.001)。将这些生物标志物纳入预测微量白蛋白尿的传统临床风险模型中,曲线下面积(AUC)从0.638增加到0.760(<0.001)。
在2型糖尿病患者中,血浆CXCL-16、血管生成素-2和TGF-β1水平升高可独立预测微量白蛋白尿。因此,这些血清标志物可改善基于既定临床危险因素的肾脏风险模型。