Ziv-Baran Tomer, Zelman Richard B, Dombrowski Philip, Schaub Amber E, Mohr Rephael, Loberman Dan
Department of Epidemiology and Preventive Medicine, School of Public Health, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Cape Cod Hospital, Hyannis, MA, USA.
Medicine (Baltimore). 2019 Nov;98(45):e17915. doi: 10.1097/MD.0000000000017915.
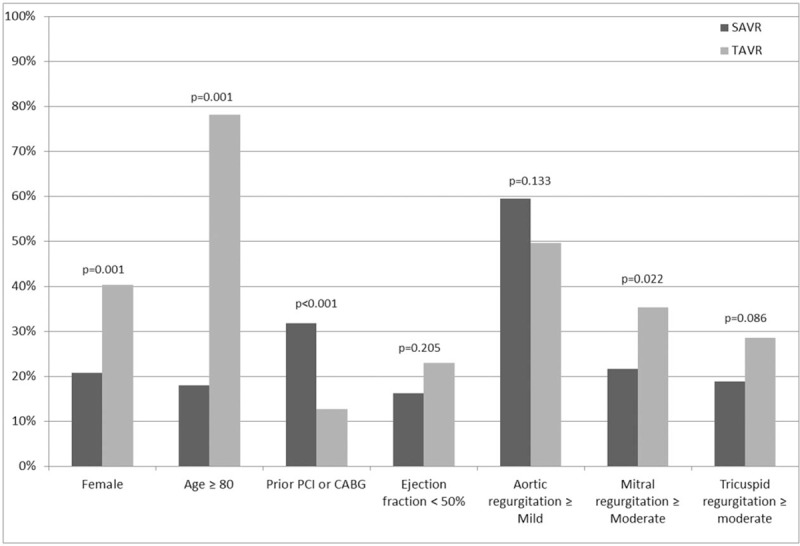
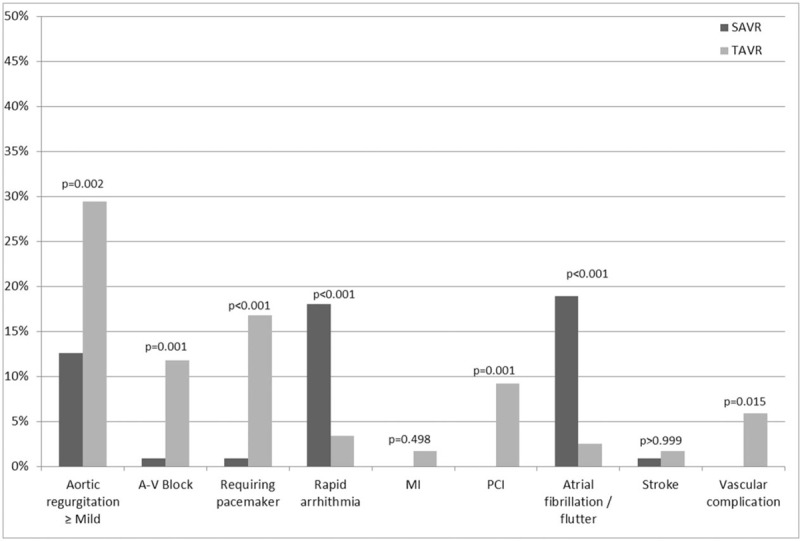
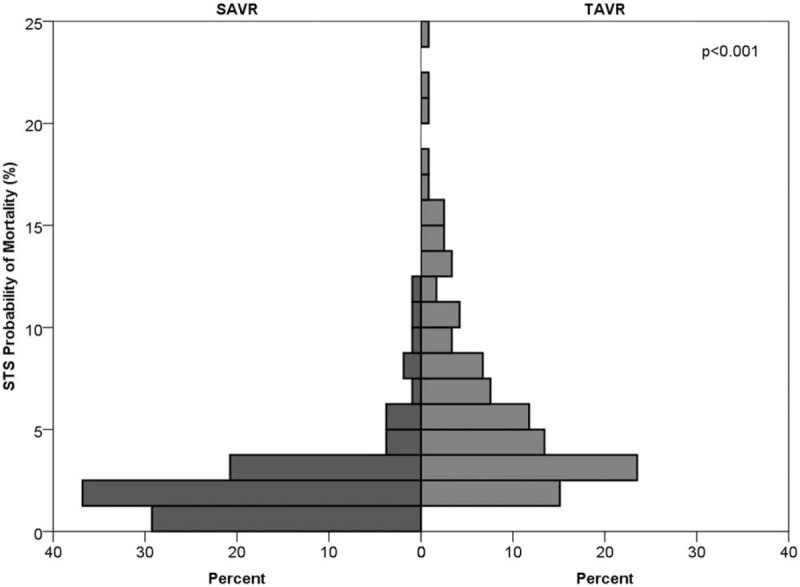
Trans-catheter aortic valve replacement (TAVR) has become an alternative to surgical aortic valve replacement (SAVR) in high and intermediate risk patients with aortic stenosis. TAVR programs are spreading from large referral centers and being established in community based institutions. The purpose of this study was to compare the outcomes of TAVR to those of SAVR in a community hospital.A historical cohort study of patients with aortic stenosis and pre-post procedure echocardiography data who underwent SAVR or TAVR in Cape Cod Hospital between January 2014 and December 2016. Patient characteristics and procedure outcomes were compared between the two procedures.The study included 230 patients, of them 111 underwent SAVR and 119 underwent TAVR. None of the patients died during the 30 days after the procedure. TAVR patients had higher rates of postoperative mild+ aortic regurgitation (AR) (29.4% vs 12.6%, P = .002), postoperative atrial ventricular blocks (11.8% vs 0.9%, P = .001), and more often need an implantation of pacemaker (16.8% vs 0.9%, P < .001). Postoperative mean gradient of SAVR patients was higher (median 14 vs 11 mm Hg, P = .001) and atrial fibrillation postoperatively was more frequent (18.9% vs 2.5%, P < .001). Length of stay after procedure was shorter in TAVR patients (median 2 vs 4 days, P < .001).After controlling for confounders, the use of TAVR was associated with an increased risk for postoperative pacemaker implantation (OR = 16.3, 95%CI 1.91-138.7, P = .011), lower mean gradient (-4.327, 95%CI -7.68 to -0.98, P = .011), and lower risk for atrial fibrillation (OR = 0.11, 95%CI 0.03-0.38, P = .001), but not with postoperative AR (OR = 0.84, 95%CI 0.22-3.13, P = .789).In conclusion, short-term mortality was not reported in SAVR or TAVR patients. However, TAVR was associated with an increased risk for postoperative pacemaker implantation but with a lower risk for atrial fibrillation. Aortic valves implanted through a trans-catheter approach are also associated with a better hemodynamic performance.
经导管主动脉瓣置换术(TAVR)已成为中高危主动脉瓣狭窄患者外科主动脉瓣置换术(SAVR)的替代方案。TAVR项目正从大型转诊中心推广开来,并在社区医疗机构中逐步建立。本研究的目的是比较在一家社区医院中TAVR与SAVR的治疗效果。
一项对2014年1月至2016年12月期间在科德角医院接受SAVR或TAVR治疗且有术前及术后超声心动图数据的主动脉瓣狭窄患者的历史性队列研究。比较了两种手术的患者特征和手术效果。
该研究纳入了230例患者,其中111例接受了SAVR,119例接受了TAVR。术后30天内无患者死亡。TAVR患者术后轻度及以上主动脉瓣反流(AR)发生率更高(29.4%对12.6%,P = 0.002),术后房室传导阻滞发生率更高(11.8%对0.9%,P = 0.001),且更常需要植入起搏器(16.8%对0.9%,P < 0.001)。SAVR患者术后平均压差更高(中位数14对11 mmHg,P = 0.001),术后房颤更常见(18.9%对2.5%,P < 0.001)。TAVR患者术后住院时间更短(中位数2天对4天,P < 0.001)。
在控制混杂因素后,使用TAVR与术后起搏器植入风险增加相关(OR = 16.3,95%CI 1.91 - 138.7,P = 0.011),平均压差更低(-4.327,95%CI -7.68至-0.98,P = 0.011),房颤风险更低(OR = 0.11,95%CI 0.03 - 0.38,P = 0.001),但与术后AR无关(OR = 0.84,95%CI 0.22 - 3.13,P = 0.789)。
总之,SAVR或TAVR患者均未报告短期死亡率。然而,TAVR与术后起搏器植入风险增加相关,但房颤风险较低。通过经导管途径植入的主动脉瓣也具有更好的血流动力学性能。