Hawkins Robert B, Downs Emily A, Johnston Lily E, Mehaffey J Hunter, Fonner Clifford E, Ghanta Ravi K, Speir Alan M, Rich Jeffrey B, Quader Mohammed A, Yarboro Leora T, Ailawadi Gorav
Division of Thoracic and Cardiovascular Surgery, Department of Surgery, University of Virginia, Charlottesville, Virginia.
Virginia Cardiac Services Quality Initiative, Falls Church, Virginia.
Ann Thorac Surg. 2017 Jun;103(6):1815-1823. doi: 10.1016/j.athoracsur.2017.02.039. Epub 2017 Apr 24.
Transcatheter aortic valve replacement (TAVR) represents a disruptive technology that is rapidly expanding in use. We evaluated the effect on surgical aortic valve replacement (SAVR) patient selection, outcomes, volume, and cost.
A total of 11,565 patients who underwent SAVR, with or without coronary artery bypass grafting (2002 to 2015), were evaluated from the Virginia Cardiac Services Quality Initiative database. Patients were stratified by surgical era: pre-TAVR era (2002 to 2008, n = 5,113), early-TAVR era (2009 to 2011, n = 2,709), and commercial-TAVR era (2012 to 2015, n = 3,743). Patient characteristics, outcomes, and resource utilization were analyzed by univariate analyses.
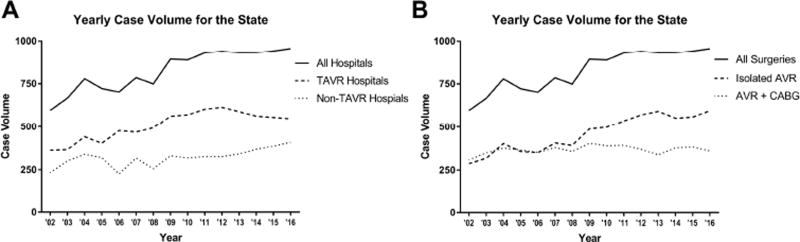
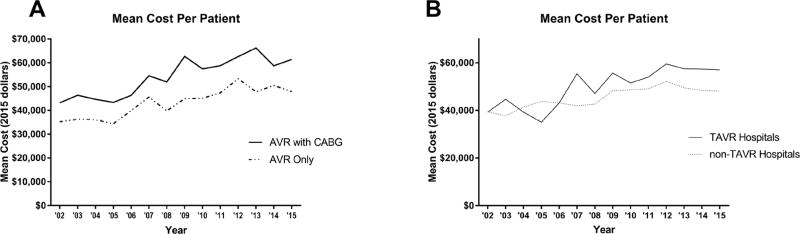
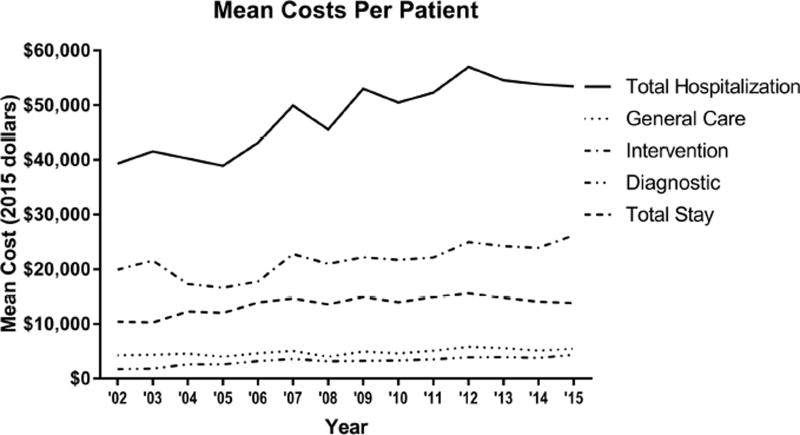
Throughout the study period, statewide SAVR volumes increased with median volumes of pre-TAVR: 722 cases/year, early-TAVR: 892 cases/year, and commercial-TAVR: 940 cases/year (p = 0.005). Implementation of TAVR was associated with declining Society of Thoracic Surgeons predicted risk of mortality among SAVR patients (3.7%, 2.6%, and 2.4%; p < 0.0001), despite increasing rates of comorbid disease. The mortality rate was lowest in the current commercial-TAVR era (3.9%, 4.3%, and 3.2%; p = 0.05), and major morbidity decreased throughout the time period (21.2%, 20.5%, and 15.2%; p < 0.0001). The lowest observed-to-expected ratios for both occurred in the commercial-TAVR era (0.9 and 0.9, respectively). Resource utilization increased generally, including total cost increases from $42,835 to $51,923 to $54,710 (p < 0.0001).
At present, SAVR volumes have not been affected by the introduction of TAVR. The outcomes for SAVR continue to improve, potentially due to availability of transcatheter options for high-risk patients. Despite rising costs for SAVR, open approaches still provide a significant cost advantage over TAVR.
经导管主动脉瓣置换术(TAVR)是一项颠覆性技术,其应用正在迅速扩展。我们评估了TAVR对外科主动脉瓣置换术(SAVR)患者选择、结局、手术量和成本的影响。
从弗吉尼亚心脏服务质量倡议数据库中评估了2002年至2015年期间共11565例行SAVR(无论是否行冠状动脉旁路移植术)的患者。患者按手术时代分层:TAVR前时代(2002年至2008年,n = 5113)、TAVR早期时代(2009年至2011年,n = 2709)和TAVR商业化时代(2012年至2015年,n = 3743)。通过单因素分析对患者特征、结局和资源利用情况进行分析。
在整个研究期间,全州范围内SAVR的手术量有所增加,TAVR前时代的中位数手术量为每年722例,TAVR早期时代为每年892例,TAVR商业化时代为每年940例(p = 0.005)。TAVR的实施与胸外科医师协会预测的SAVR患者死亡率下降相关(分别为3.7%、2.6%和2.4%;p < 0.0001),尽管合并症发生率有所上升。当前TAVR商业化时代的死亡率最低(分别为3.9%、4.3%和3.2%;p = 0.05),且在此期间主要并发症发生率下降(分别为21.2%、20.5%和15.2%;p < 0.0001)。两者观察到的与预期的比率最低均出现在TAVR商业化时代(分别为0.9和0.9)。资源利用总体上有所增加,包括总成本从42835美元增加到51923美元再增加到54710美元(p < 0.0001)。
目前,SAVR的手术量未受TAVR引入的影响。SAVR的结局持续改善,这可能是由于为高危患者提供了经导管治疗选择。尽管SAVR成本上升,但开放手术方法仍比TAVR具有显著的成本优势。