Department of Orthopaedics, The Second Affiliated Hospital of Soochow University, 1055 Sanxiang Road, Suzhou, 215006, China.
Department of Orthopaedics, Binzhou Central Hospital Affiliated to Binzhou Medical University, 108 Huancheng South Road, Huimin, Binzhou, 251700, Shandong, China.
J Orthop Surg Res. 2019 Nov 8;14(1):347. doi: 10.1186/s13018-019-1374-8.
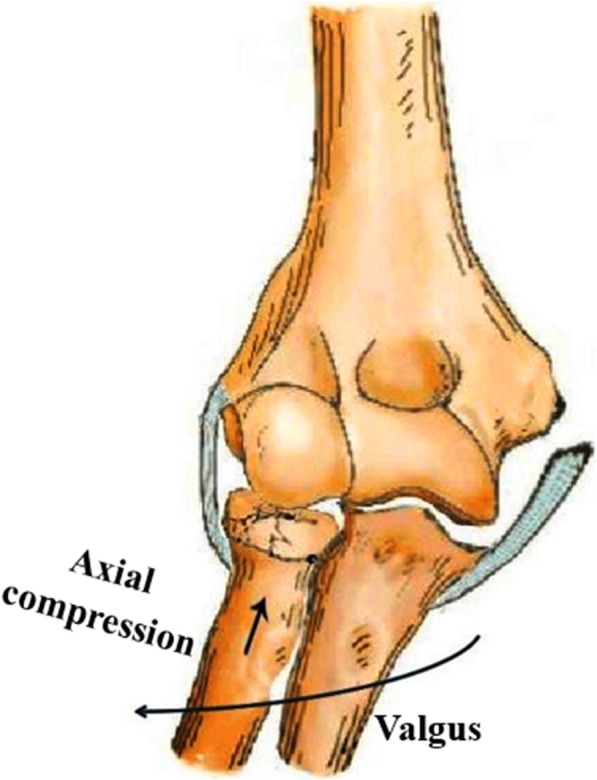
The objective of the study was to depict the pathoanatomy of traumatic valgus instability of the elbow and to report clinical outcomes of primary operation.
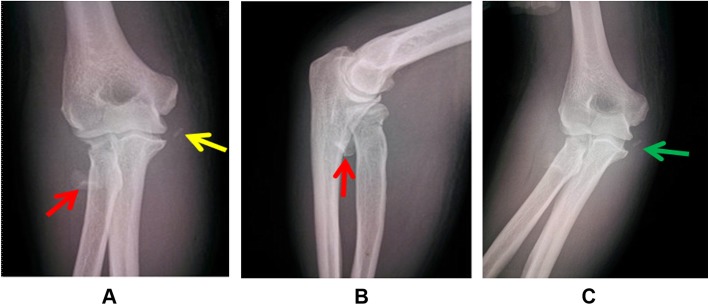
Thirty-one patients presented with traumatic valgus instability of the elbow without dislocation. Thirty-one patients underwent surgical intervention of radial head fractures (28 open reduction and internal fixation and 3 radial head resection) and anatomical repair of the anterior bundle of medial collateral ligament (AMCL) with suture anchors. Twenty patients with disruption of the flexor-pronator tendon (FPT) and 14 patients with tears of the anterior capsule had primary repair of the FPT and anterior capsule simultaneously. Clinical outcomes were evaluated with the Mayo Elbow Performance Score (MEPS), modified hospital for special surgery assessment scale (HSS), and Disabilities of the Arm, Shoulder, and Hand (DASH) score.
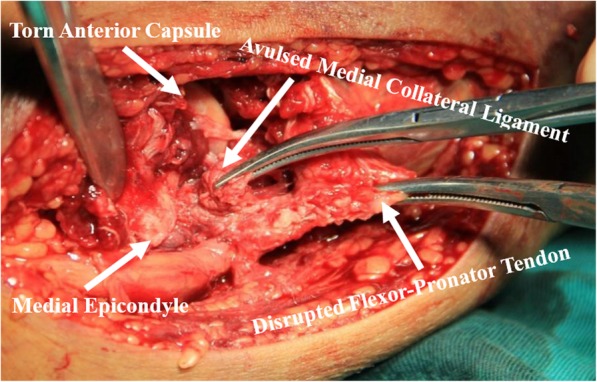
The median follow-up was 37.3 months (range, 15-53 months). Radial head fractures and complete avulsion of the medial collateral ligament (MCL) from its humeral footprint were confirmed in all patients intraoperatively. Intraoperative findings indicated disruption of the FPT in 20 patients and tears of the anterior capsule in 14 patients. Twenty-nine of 31 patients returned to previous activity and work levels within 6 months after surgery. The MEPS, modified HSS, and DASH score were 94 ± 4, 91 ± 5, and 8 ± 2 at the latest follow-up.
Radial head fractures with avulsion of the MCL can lead to severe valgus instability of the elbow. Primary operation to repair these disrupted structures, especially repair of the AMCL, can effectively restore valgus stability.
本研究旨在描述创伤性肘外翻不稳定的病理解剖结构,并报告初次手术的临床结果。
31 例患者均为创伤性肘外翻不稳定且无脱位。31 例患者接受了桡骨头骨折的手术干预(28 例切开复位内固定和 3 例桡骨头切除)和内侧副韧带前束(AMCL)解剖修复,使用缝合锚钉。20 例屈肌-旋前肌腱(FPT)断裂和 14 例前关节囊撕裂的患者同时进行 FPT 和前关节囊的初次修复。采用 Mayo 肘功能评分(MEPS)、改良的特种外科医院(HSS)评分和上肢残疾问卷(DASH)评分评估临床结果。
中位随访时间为 37.3 个月(范围,15-53 个月)。所有患者术中均证实存在桡骨头骨折和 AMCL 从肱骨附着点完全撕脱。术中发现 20 例 FPT 断裂,14 例前关节囊撕裂。31 例患者中有 29 例在术后 6 个月内恢复到术前的活动和工作水平。末次随访时 MEPS、改良 HSS 和 DASH 评分分别为 94±4、91±5 和 8±2。
桡骨头骨折伴 AMCL 撕脱可导致严重的肘外翻不稳定。修复这些受损结构,尤其是修复 AMCL,可有效恢复外翻稳定性。