Department of Clinical Sciences, Lund University/Clinical Research Centre, Skåne University Hospital, Malmö, Sweden.
Institute of Biomedical and Clinical Science, University of Exeter Medical School, Exeter, U.K.
Diabetes Care. 2020 Jan;43(1):82-89. doi: 10.2337/dc19-0747. Epub 2019 Nov 8.
Identifying maturity-onset diabetes of the young (MODY) in pediatric populations close to diabetes diagnosis is difficult. Misdiagnosis and unnecessary insulin treatment are common. We aimed to identify the discriminatory clinical features at diabetes diagnosis of patients with glucokinase (GCK), hepatocyte nuclear factor-1A (HNF1A), and HNF4A MODY in the pediatric population.
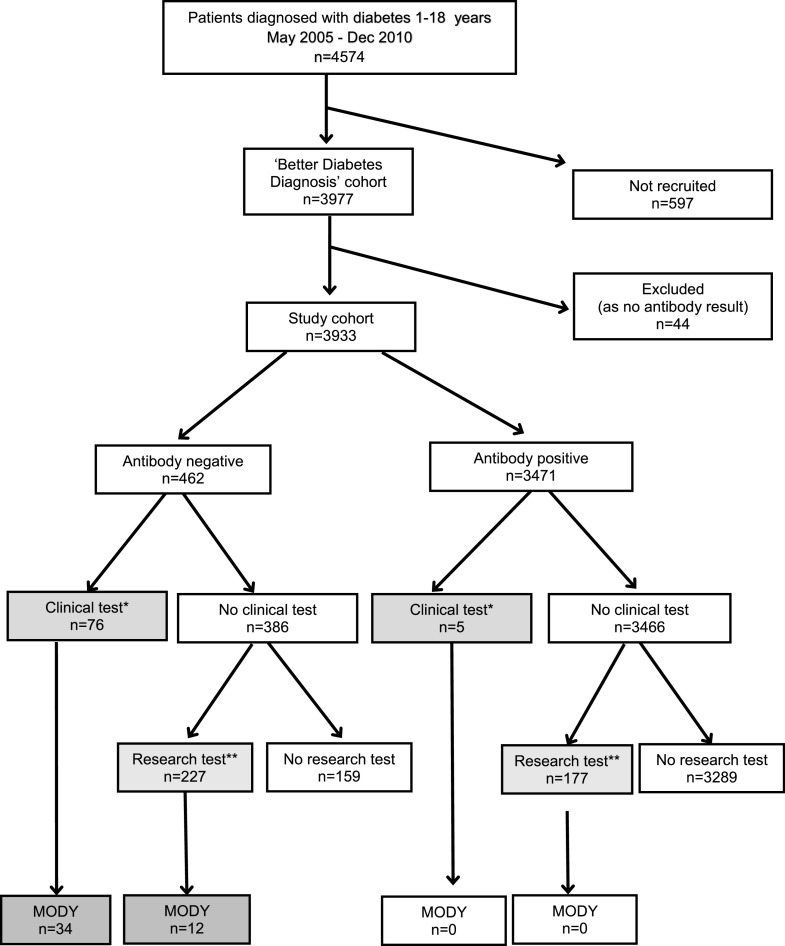
Swedish patients ( = 3,933) aged 1-18 years, diagnosed with diabetes May 2005 to December 2010, were recruited from the national consecutive prospective cohort Better Diabetes Diagnosis. Clinical data, islet autoantibodies (GAD insulinoma antigen-2, zinc transporter 8, and insulin autoantibodies), HLA type, and C-peptide were collected at diagnosis. MODY was identified by sequencing , , and , through either routine clinical or research testing.
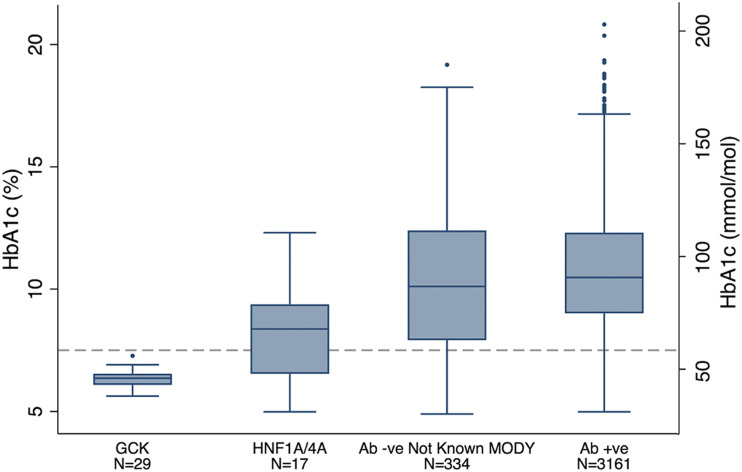
The minimal prevalence of MODY was 1.2%. Discriminatory factors for MODY at diagnosis included four islet autoantibody negativity (100% vs. 11% not-known MODY; = 2 × 10), HbA (7.0% vs. 10.7% [53 vs. 93 mmol/mol]; = 1 × 10), plasma glucose (11.7 vs. 26.7 mmol/L; = 3 × 10), parental diabetes (63% vs. 12%; = 1 × 10), and diabetic ketoacidosis (0% vs. 15%; = 0.001). Testing 303 autoantibody-negative patients identified 46 patients with MODY (detection rate 15%). Limiting testing to the 73 islet autoantibody-negative patients with HbA <7.5% (58 mmol/mol) at diagnosis identified 36 out of 46 (78%) patients with MODY (detection rate 49%). On follow-up, the 46 patients with MODY had excellent glycemic control, with an HbA of 6.4% (47 mmol/mol), with 42 out of 46 (91%) patients not on insulin treatment.
At diagnosis of pediatric diabetes, absence of all islet autoantibodies and modest hyperglycemia (HbA <7.5% [58 mmol/mol]) should result in testing for GCK, HNF1A, and HNF4A MODY. Testing all 12% patients negative for four islet autoantibodies is an effective strategy for not missing MODY but will result in a lower detection rate. Identifying MODY results in excellent long-term glycemic control without insulin.
在接近糖尿病诊断的儿科人群中识别青少年发病的成年型糖尿病(MODY)较为困难。误诊和不必要的胰岛素治疗较为常见。本研究旨在鉴定在儿科人群中葡萄糖激酶(GCK)、肝细胞核因子-1A(HNF1A)和 HNF4A MODY 患者糖尿病诊断时具有鉴别意义的临床特征。
2005 年 5 月至 2010 年 12 月,我们从全国连续前瞻性队列研究“更好的糖尿病诊断”中招募了年龄在 1-18 岁、新诊断为糖尿病的瑞典患者(n=3933)。在诊断时收集了临床数据、胰岛自身抗体(谷氨酸脱羧酶、胰岛素瘤抗原-2、锌转运体 8 和胰岛素自身抗体)、HLA 类型和 C 肽。通过常规临床或研究检测,对 、 、 和 进行测序以确定 MODY。
MODY 的最小患病率为 1.2%。MODY 诊断时的鉴别因素包括四项胰岛自身抗体阴性(100% vs. 11%未知 MODY; = 2 × 10)、糖化血红蛋白(7.0% vs. 10.7%[53 vs. 93 mmol/mol]; = 1 × 10)、血浆葡萄糖(11.7 vs. 26.7 mmol/L; = 3 × 10)、父母糖尿病(63% vs. 12%; = 1 × 10)和糖尿病酮症酸中毒(0% vs. 15%; = 0.001)。对 303 名自身抗体阴性患者进行检测,鉴定出 46 名 MODY 患者(检出率 15%)。将检测限制在诊断时糖化血红蛋白(HbA)<7.5%(58 mmol/mol)且自身抗体阴性的 73 名患者中,鉴定出 46 名 MODY 患者中的 36 名(78%;检出率 49%)。在随访中,46 名 MODY 患者的血糖控制良好,HbA 为 6.4%(47 mmol/mol),其中 42 名(91%)患者无需胰岛素治疗。
在儿科糖尿病患者的诊断中,如果四项胰岛自身抗体均为阴性且存在轻度高血糖(HbA<7.5%[58 mmol/mol]),则应进行 GCK、HNF1A 和 HNF4A MODY 检测。对 12%的四项胰岛自身抗体阴性患者进行所有检测是一种有效的策略,不会漏诊 MODY,但检出率较低。确定 MODY 后,可实现长期良好的血糖控制,无需胰岛素治疗。