Cardiology Unit, Cardio-Thoracic-Vascular Department, Sant'Orsola-Malpighi Hospital, University of Bologna, Via G. Massarenti 9, 40138, Bologna, Italy.
Cardiology Division, Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Policlinico di Modena, Modena, Italy.
Orphanet J Rare Dis. 2019 Nov 19;14(1):263. doi: 10.1186/s13023-019-1245-8.
To investigate differences in cardiac manifestations of patients affected by laminopathy, according to the presence or absence of neuromuscular involvement at presentation.
We prospectively analyzed 40 consecutive patients with a diagnosis of laminopathy followed at a single centre between 1998 and 2017. Additionally, reports of clinical evaluations and tests prior to referral at our centre were retrospectively evaluated.
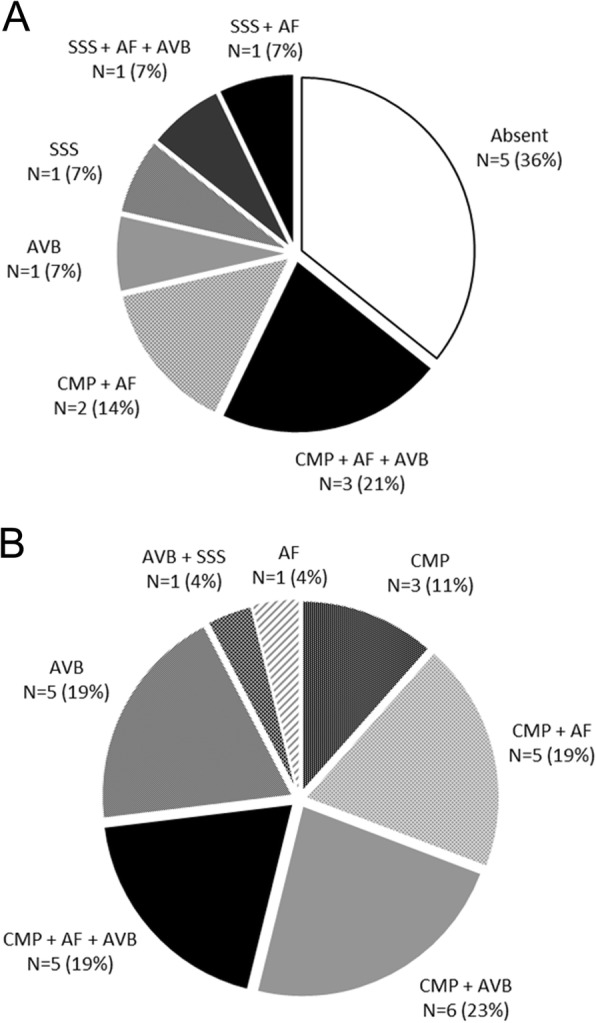
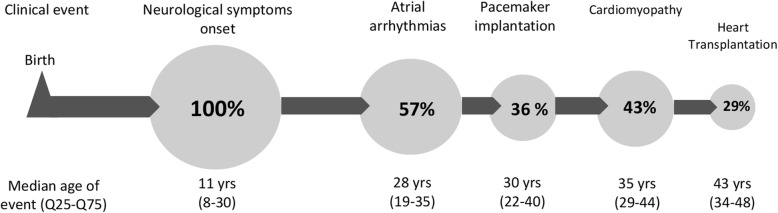
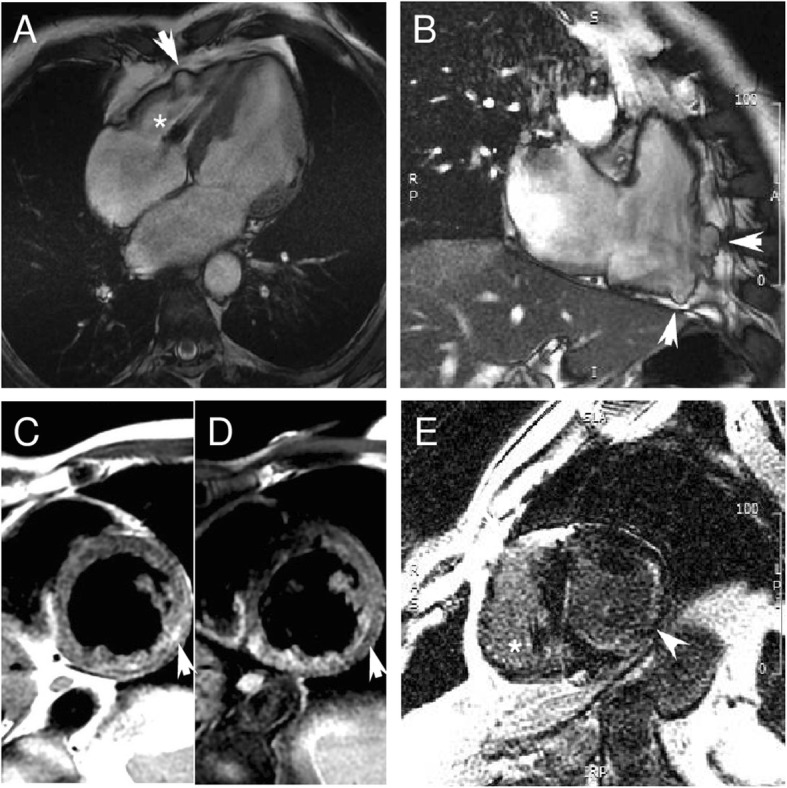
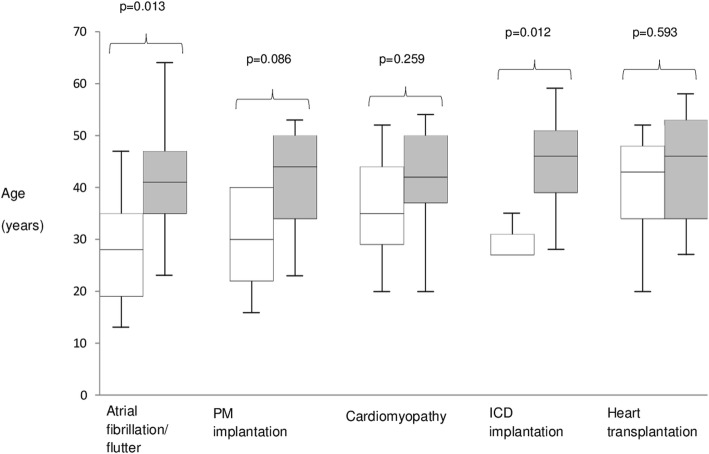
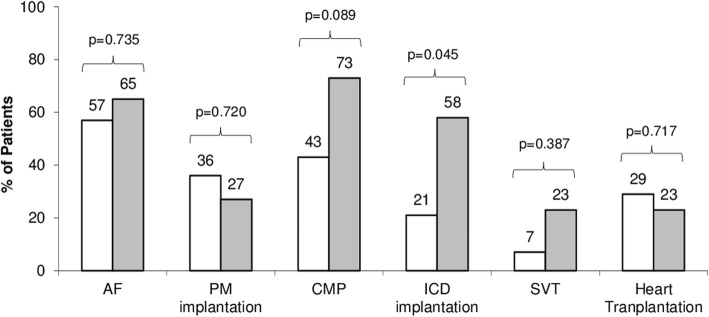
Clinical onset was cardiac in 26 cases and neuromuscular in 14. Patients with neuromuscular presentation experienced first symptoms earlier in life (11 vs 39 years; p < 0.0001) and developed atrial fibrillation/flutter (AF) and required pacemaker implantation at a younger age (28 vs 41 years [p = 0.013] and 30 vs 44 years [p = 0.086] respectively), despite a similar overall prevalence of AF (57% vs 65%; p = 0.735) and atrio-ventricular (A-V) block (50% vs 65%; p = 0.500). Those with a neuromuscular presentation developed a cardiomyopathy less frequently (43% vs 73%; p = 0.089) and had a lower rate of sustained ventricular tachyarrhythmias (7% vs 23%; p = 0.387). In patients with neuromuscular onset rhythm disturbances occurred usually before evidence of cardiomyopathy. Despite these differences, the need for heart transplantation and median age at intervention were similar in the two groups (29% vs 23% [p = 0.717] and 43 vs 46 years [p = 0.593] respectively).
In patients with laminopathy, the type of disease onset was a marker for a different natural history. Specifically, patients with neuromuscular presentation had an earlier cardiac involvement, characterized by a linear and progressive evolution from rhythm disorders (AF and/or A-V block) to cardiomyopathy.
研究在呈现时是否存在神经肌肉受累,对受层状蛋白病影响的患者的心脏表现的差异。
我们前瞻性分析了 1998 年至 2017 年间在一家中心接受诊断为层状蛋白病的连续 40 例患者。此外,还回顾性评估了在我们中心转诊前的临床评估和检查报告。
26 例患者首发症状为心脏,14 例患者首发症状为神经肌肉。有神经肌肉表现的患者更早出现首发症状(11 岁 vs 39 岁;p<0.0001),并更早出现心房颤动/扑动(AF)和需要植入起搏器(28 岁 vs 41 岁[p=0.013]和 30 岁 vs 44 岁[p=0.086]),尽管 AF(57% vs 65%;p=0.735)和房室(A-V)传导阻滞(50% vs 65%;p=0.500)的总体发生率相似。有神经肌肉表现的患者较少发生心肌病(43% vs 73%;p=0.089),持续性室性心律失常的发生率也较低(7% vs 23%;p=0.387)。有神经肌肉起病的患者,心律失常通常先于心肌病的证据出现。尽管存在这些差异,但两组患者需要心脏移植和干预的中位年龄相似(29% vs 23%[p=0.717]和 43 岁 vs 46 岁[p=0.593])。
在层状蛋白病患者中,疾病发作的类型是不同自然病史的标志物。具体来说,有神经肌肉表现的患者心脏受累更早,表现为节律障碍(AF 和/或 A-V 传导阻滞)至心肌病的线性和进行性进展。