Manson Unit, Médecins sans Frontières, London, UK
Centre for Global Chronic Conditions, Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, UK.
BMJ Open. 2019 Nov 24;9(11):e030176. doi: 10.1136/bmjopen-2019-030176.
We aimed to evaluate an Integrated Diabetic Clinic within a Hospital Outpatient Department (IDC-OPD) in a complex humanitarian setting in North Kivu, Democratic Republic of Congo. Specific objectives were to: (1) analyse diabetes intermediate clinical and programmatic outcomes (blood pressure (BP)/glycaemic control, visit volume and frequency); (2) explore the association of key insecurity and related programmatic events with these outcomes; and (3) describe incremental IDC-OPD programme costs.
Retrospective cohort analysis of routine programmatic data collected from January 2014 to February 2017; analysis of programme costs for 2014/2015.
Outpatient diabetes programme in Mweso hospital, supported by Médecins sans Frontières, in North Kivu, Demographic Republic of Congo.
Diabetes patients attending IDC-OPD.
Intermediate clinical and programmatic outcome trends (BP/ glycaemic control; visit volume/frequency); incremental programme costs.
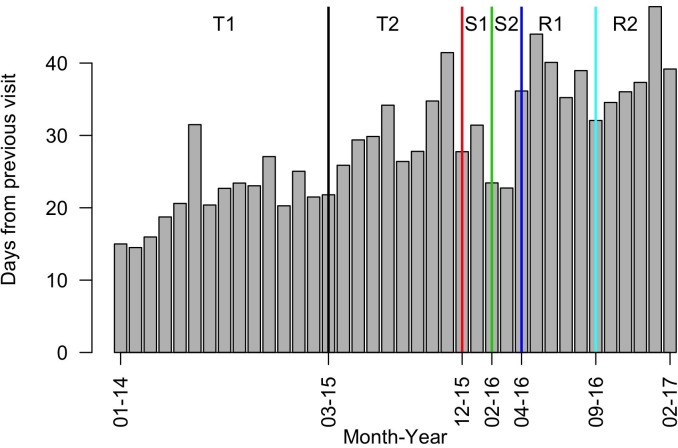
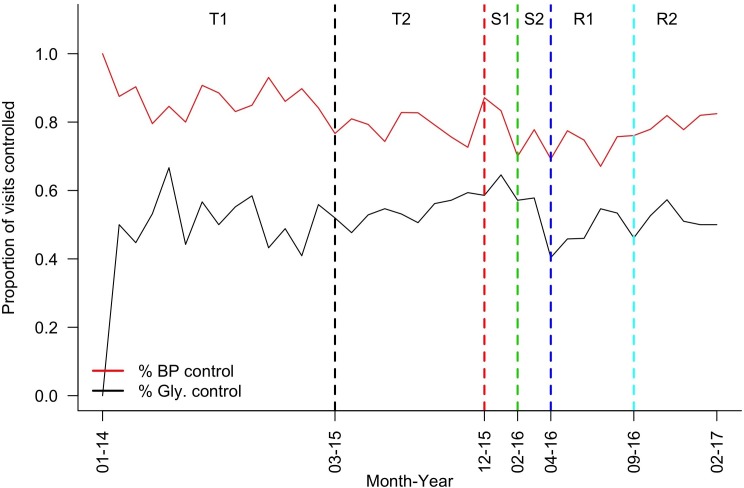
Of 243 diabetes patients, 44.6% were women, median age was 45 (IQR 32-56); 51.4% were classified type 2. On introduction of IDC-OPD, glucose control improved and patient volume and visit interval increased. During insecurity, control rates were initially maintained by a nurse-provided, scaled-back service, while patient volume and visit interval decreased. Following service suspension due to drug stock-outs, patients were less likely to achieve control, improving on service resumption. Total costs decreased 16% from 2014 (€36 573) to 2015 (€30 861). Annual cost per patient dropped from €475 in 2014 to €214 in 2015 due to reduced supply costs and increased patient numbers.
In a chronic conflict setting, we documented that control of diabetes intermediate outcomes was achievable during stable periods. During insecure periods, a simplified, nurse-led model maintained control rates until drug stock-outs occurred. Incremental per patient annual costs were lower than chronic HIV care costs in low-income settings. Future operational research should define a simplified diabetes care package including emergency preparedness.
我们旨在评估北基伍民主刚果一个复杂人道主义环境下的医院门诊部内的综合糖尿病诊所(IDC-OPD)。具体目标是:(1)分析糖尿病中间临床和项目成果(血压(BP)/血糖控制、就诊量和就诊频率);(2)探索关键不安全因素及相关项目事件与这些结果的关联;(3)描述 IDC-OPD 项目成本的增量。
2014 年 1 月至 2017 年 2 月期间,从常规项目数据中进行回顾性队列分析;2014/2015 年对项目成本进行分析。
北基伍民主刚果姆韦索医院的门诊糖尿病项目,由无国界医生组织提供支持。
在 IDC-OPD 就诊的糖尿病患者。
243 名糖尿病患者中,44.6%为女性,中位年龄为 45 岁(IQR 32-56);51.4%为 2 型糖尿病患者。引入 IDC-OPD 后,血糖控制得到改善,就诊量和就诊间隔增加。在不安全期间,最初通过护士提供的缩减服务来维持控制率,而就诊量和就诊间隔减少。由于药物库存耗尽而暂停服务后,患者控制率降低,在服务恢复后有所改善。总成本从 2014 年的 36573 欧元下降到 2015 年的 30861 欧元,降幅为 16%。由于供应成本降低和就诊人数增加,每位患者的年费用从 2014 年的 475 欧元降至 2015 年的 214 欧元。
在慢性冲突环境下,我们记录了在稳定时期可以实现糖尿病中间结果的控制。在不安全时期,简化的、由护士主导的模式可以维持控制率,直到药物库存耗尽。每位患者的年度增量成本低于低收入环境下慢性 HIV 护理的成本。未来的运营研究应确定包括应急准备的简化糖尿病护理方案。