Department of Pediatrics, Division of Pediatric Cardiology, Duke University Medical Center, Durham, North Carolina.
Catheter Cardiovasc Interv. 2020 May 1;95(6):1141-1148. doi: 10.1002/ccd.28669. Epub 2019 Dec 18.
Describe the use of three-dimensional (3D) patent ductus arteriosus (PDA) modeling to better define ductal anatomy to improve preprocedural planning for ductal stent placement.
Ductal stenting is an alternative to surgical shunting in patients with ductal dependent pulmonary blood flow. Ductal anatomy is often complex with extreme tortuosity and risk of pulmonary artery isolation, thus increasing procedural risks.
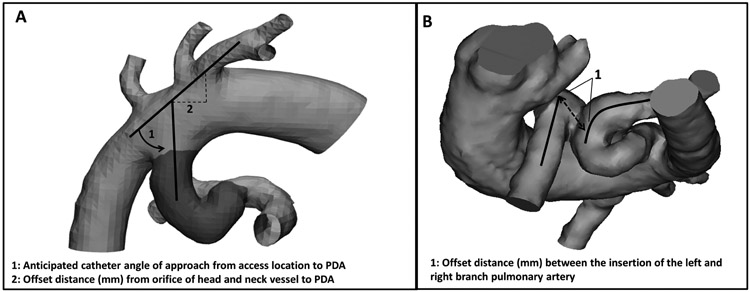
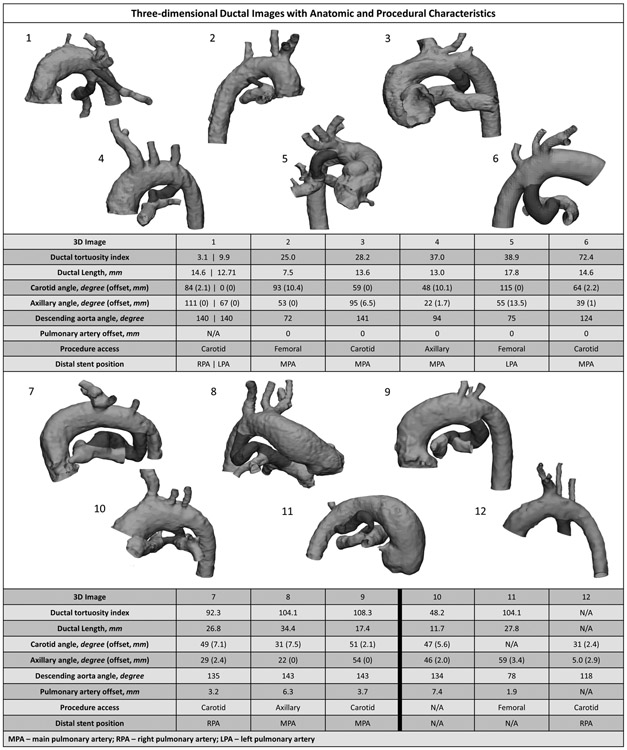
CT angiograms were segmented to produce 3D PDA models. Ductal morphology was characterized with attention to access approach, degree of pulmonary artery offset/risk of isolation and ductal tortuosity. 3D models were retrospectively compared with biplane angiography.
3D modeling was performed in 12 patients with adequate image quality for complete analysis in 11; median (interquartile range) age/weight 17 days (8-20 days) and 3.1 kg (2.4-3.9 kg). The PDA was reverse oriented in nine with average length of 17.2 ± 2.5 mm and high tortuosity (mean tortuosity index 52, range 3-108). From 3D modeling, two patients were excluded from ductal stenting-extreme ductal tortuosity and threatened pulmonary artery discontinuity, respectively. Ductal stenting was successful in the remaining nine with no major procedural complications. 3D modeling predicted a successful access approach based on the aortic orientation of the ductus in all patients (five carotid, two axillary, two femoral). When comparing 2D angiography with 3D models, angiography consistently underestimated ductal length (-3.2 mm ± 1.6 mm) and tortuosity (-14.8 ± 7.2).
3D modeling prior to ductal stent placement for ductal dependent pulmonary blood flow is useful in procedural planning, specifically for eligibility, access approach, and accurate ductal measurements. Further studies are needed to determine if 3D planning improves procedural outcomes.
描述使用三维(3D)动脉导管未闭(PDA)模型来更好地定义导管解剖结构,从而改进导管支架置入的术前规划。
在依赖导管的肺血流量患者中,导管支架置入是一种替代手术分流的方法。导管解剖结构通常非常复杂,具有极度迂曲和肺动脉隔离的风险,从而增加了手术风险。
对 CT 血管造影进行分割以生成 3D PDA 模型。注意导管的入路途径、肺动脉偏移程度/隔离风险和导管迂曲程度来描述导管形态。将 3D 模型与双平面血管造影进行回顾性比较。
12 例患者进行了 3D 建模,11 例患者具有足够的图像质量进行完整分析;中位(四分位间距)年龄/体重为 17 天(8-20 天)和 3.1 千克(2.4-3.9 千克)。9 例患者的 PDA 呈反向排列,平均长度为 17.2±2.5 毫米,迂曲度高(平均迂曲指数 52,范围 3-108)。通过 3D 建模,两名患者分别因导管极度迂曲和肺动脉连续性受威胁而被排除在导管支架置入之外。其余 9 例患者成功进行了导管支架置入,无主要手术并发症。3D 建模根据导管在主动脉中的方向预测了所有患者(5 例颈动脉、2 例腋动脉、2 例股动脉)成功的入路途径。与 3D 模型相比,血管造影术始终低估了导管长度(-3.2 毫米±1.6 毫米)和迂曲度(-14.8±7.2)。
在依赖导管的肺血流量患者中,在进行导管支架置入之前进行 3D 建模对于手术规划非常有用,特别是对于适应证、入路途径和准确的导管测量。需要进一步的研究来确定 3D 规划是否能改善手术结果。