From the Regional Center of Knowledge Translation in Rehabilitation, Sunnaas Rehabilitation Hospital, Oslo/Nesodden, Norway (J.L.M.).
Institute for Knowledge Translation, Carmel, IN (J.L.M.).
Stroke. 2020 Feb;51(2):563-570. doi: 10.1161/STROKEAHA.119.027450. Epub 2019 Dec 30.
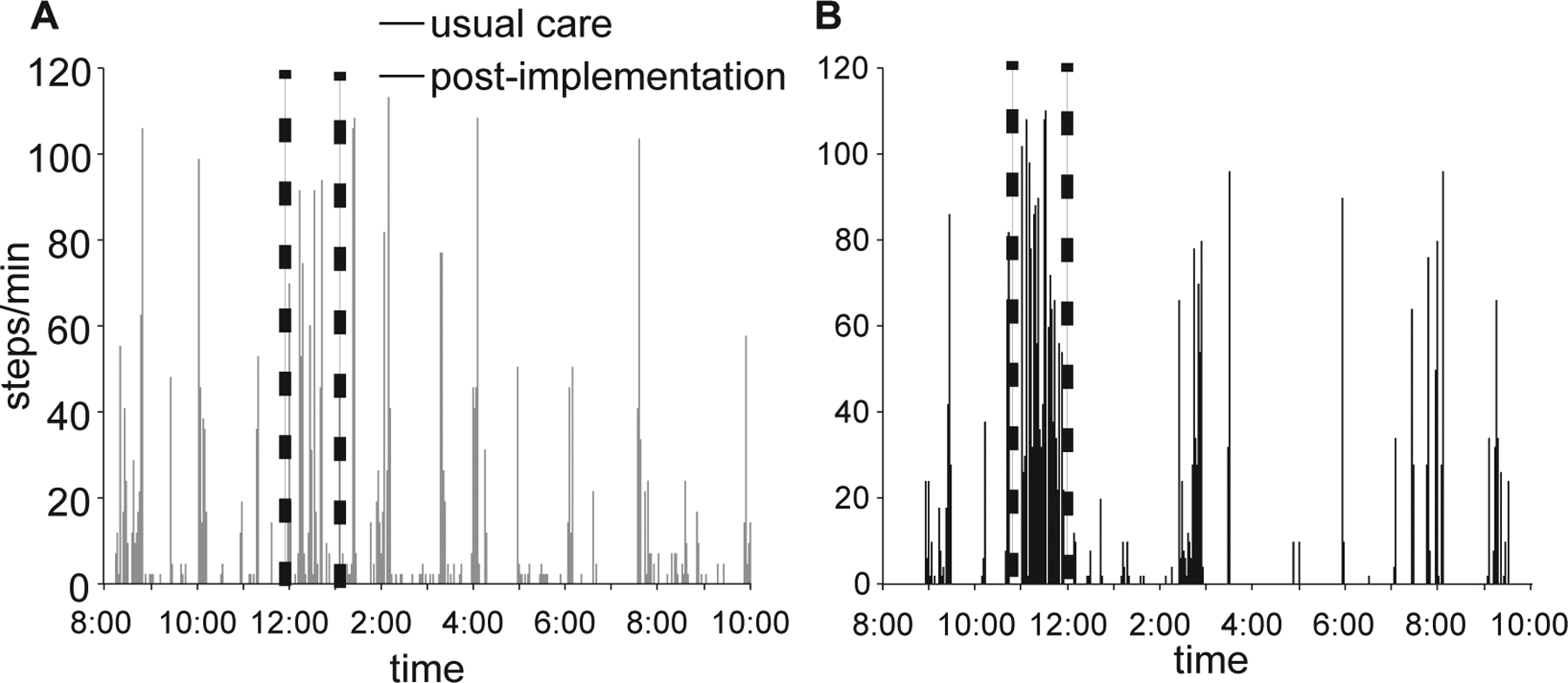
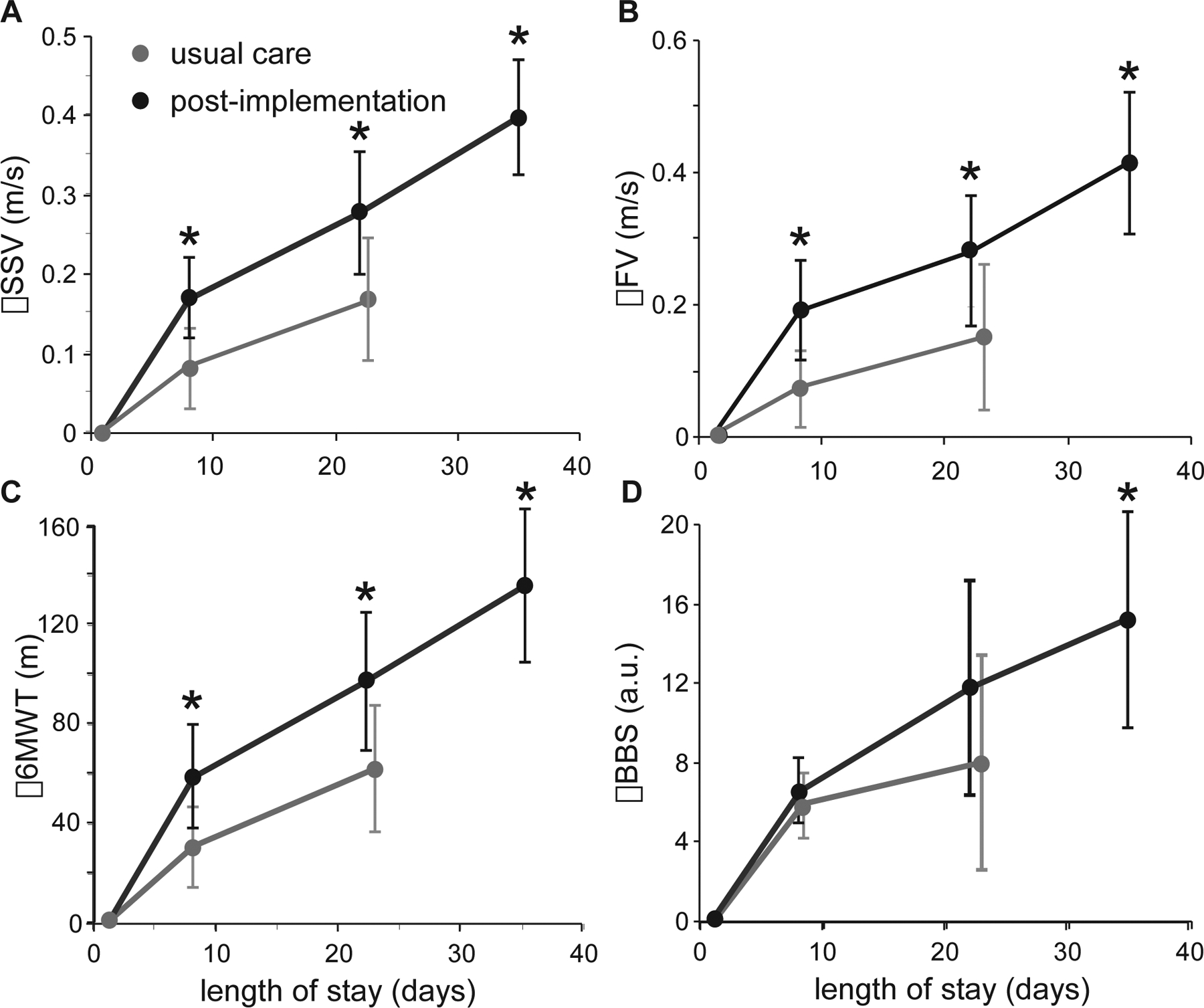
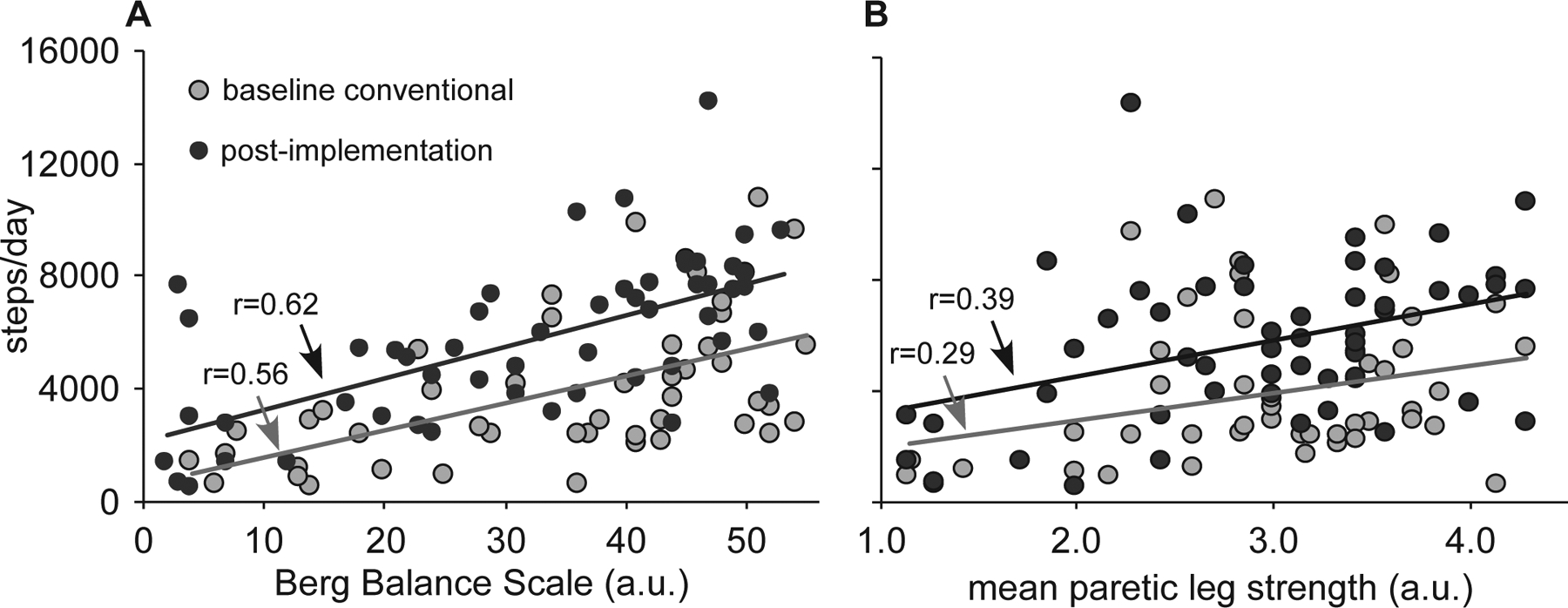
Background and Purpose- Therapeutic strategies that capitalize on the intrinsic capacity for neurological recovery early poststroke to improve locomotion are uncertain. Emerging data suggest that task-specific stepping practice provided at higher cardiovascular intensities may be critical dosage parameters that could maximize locomotor recovery. The purpose of this investigation was to determine the comparative effectiveness of providing high-intensity training on locomotor capacity early poststroke as compared with usual care. Methods- A quasi-experimental design was used to compare changes in stepping activity (StepWatch), walking, and balance outcomes during usual care (n=56) versus high-intensity stepping intervention (n=54) in inpatient stroke patients. Primary outcomes assessed weekly included self-selected and fastest gait speed, 6-minute walk test, and the Berg Balance Scale, with secondary outcomes of Swedish Postural Assessment Scale for Stroke-Norwegian version, Functional Ambulation Category, 30-s sit-to-stand, strength (average manual muscle testing), and Barthel Index. Regression analyses identified relationships between demographics, baseline function, and training activities (steps per day; duration achieved, 70%-85% maximum heart rates) and primary outcomes at discharge. Results- Following implementation of high-intensity stepping, average steps per day (5777±2784) were significantly greater than during usual care (3917±2656; <0.001). Statistically different and clinically meaningful changes in self-selected speed (0.39±0.28 versus 0.16±0.26 m/s) and fastest gait speed (0.47±0.41 versus 0.17±0.38 m/s; both <0.001) were observed following high-intensity interventions versus usual care and at every assessment throughout the length of stay. Changes in Berg Balance Scale and 6-minute walk test were also statistically and clinically different between groups, while secondary measures of Functional Ambulation Category and strength were also different at discharge. Primary predictors of improved walking capacity were steps per day, baseline impairments, and age. Conclusions- Provision of high-intensity stepping training applied during inpatient rehabilitation resulted in significantly greater walking and balance outcomes. This training paradigm should be further tested in other contexts to determine the generalizability to real-world and community settings.
背景与目的-利用中风后早期的神经固有恢复能力来改善运动功能的治疗策略尚不确定。新出现的数据表明,在较高心血管强度下提供特定于任务的踏步练习可能是关键的剂量参数,可以最大限度地提高运动功能的恢复。本研究的目的是确定与常规护理相比,早期提供高强度训练对运动能力的比较效果。方法-使用准实验设计比较了常规护理(n=56)与高强度踏步干预(n=54)中住院中风患者的踏步活动(StepWatch)、行走和平衡结果的变化。每周评估的主要结果包括自我选择的和最快的步行速度、6 分钟步行测试和 Berg 平衡量表,次要结果包括瑞典体位评估量表-挪威版本、功能性步行分类、30 秒坐站、力量(平均手动肌肉测试)和 Barthel 指数。回归分析确定了人口统计学、基线功能和训练活动(每天步数;达到的时长,70%-85%最大心率)与出院时主要结果之间的关系。结果-高强度踏步实施后,平均每天步数(5777±2784)明显大于常规护理(3917±2656;<0.001)。与常规护理相比,高强度干预组的自我选择速度(0.39±0.28 与 0.16±0.26 m/s)和最快步行速度(0.47±0.41 与 0.17±0.38 m/s;均<0.001)的变化具有统计学意义和临床意义,且在整个住院期间的每次评估中均观察到。Berg 平衡量表和 6 分钟步行测试的变化在组间也具有统计学和临床意义,而功能性步行分类和力量的次要测量指标在出院时也不同。行走能力改善的主要预测因素是每天步数、基线损伤和年龄。结论-在住院康复期间提供高强度踏步训练可显著改善行走和平衡功能。应在其他环境中进一步测试这种训练模式,以确定其在真实世界和社区环境中的普遍性。