1Department of General Surgery, Singapore General Hospital, 20 College Road, Academia Level 5, Singapore, 169856 Singapore.
2SingHealth Internal Medicine Residency, Singapore General Hospital, 20 College Road, Academia Level 3, Singapore, 169856 Singapore.
World J Emerg Surg. 2019 Dec 30;14:62. doi: 10.1186/s13017-019-0280-z. eCollection 2019.
Frailty has been associated with an increased risk of adverse postoperative outcomes in elderly patients. We examined the impact of preoperative frailty on loss of functional independence following emergency abdominal surgery in the elderly.
This prospective cohort study was performed at a tertiary hospital, enrolling patients 65 years of age and above who underwent emergency abdominal surgery from June 2016 to February 2018. Premorbid variables, perioperative characteristics and outcomes were collected. Two frailty measures were compared in this study-the Modified Fried's Frailty Criteria (mFFC) and Modified Frailty Index-11 (mFI-11). Patients were followed-up for 1 year.
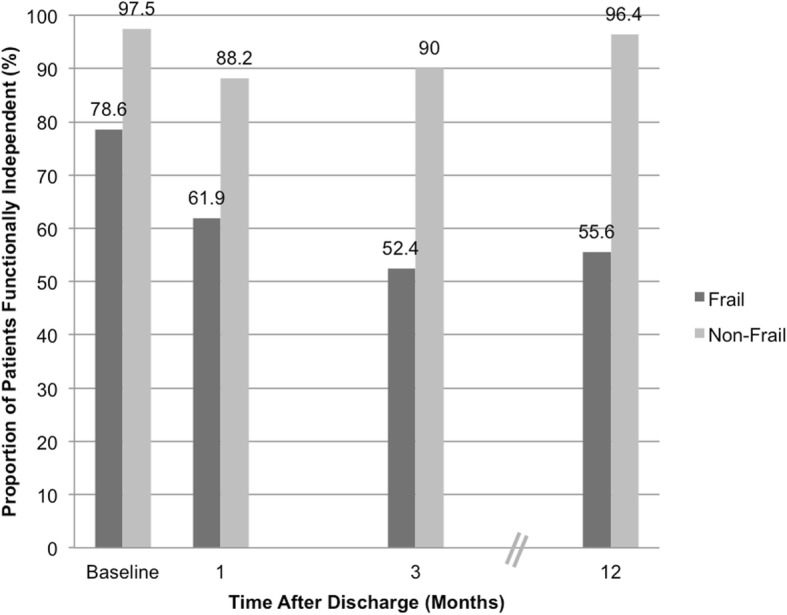
A total of 109 patients were prospectively recruited. At baseline, 101 (92.7%) were functionally independent, of whom seven (6.9%) had loss of independence at 1 year; 28 (25.7%) and 81 (74.3%) patients were frail and non-frail (by mFFC) respectively. On univariate analysis, age, Charlson Comorbidity Index and frailty (mFFC) (univariate OR 13.00, 95% CI 2.21-76.63, < 0.01) were significantly associated with loss of functional independence at 1 year. However, frailty, as assessed by mFI-11, showed a weaker correlation than mFFC (univariate OR 4.42, 95% CI 0.84-23.12, = 0.06). On multivariable analysis, only premorbid frailty (by mFFC) remained statistically significant (OR 15.63, 95% CI 2.12-111.11, < 0.01).
The mFFC is useful for frailty screening amongst elderly patients undergoing emergency abdominal surgery and is a predictor for loss of functional independence at 1 year. Including the risk of loss of functional independence in perioperative discussions with patients and caregivers is important for patient-centric emergency surgical care. Early recognition of this at-risk group could help with discharge planning and priority for post-discharge support should be considered.
虚弱与老年患者术后不良结局的风险增加有关。我们研究了术前虚弱对老年急诊腹部手术后丧失功能独立性的影响。
这项前瞻性队列研究在一家三级医院进行,纳入了 2016 年 6 月至 2018 年 2 月期间接受急诊腹部手术的 65 岁及以上的患者。收集了术前变量、围手术期特征和结局。本研究比较了两种虚弱评估方法——改良 Fried 虚弱标准(mFFC)和改良虚弱指数-11(mFI-11)。患者随访 1 年。
共前瞻性招募了 109 名患者。基线时,101 名(92.7%)患者功能独立,其中 7 名(6.9%)在 1 年内丧失独立性;28 名(25.7%)和 81 名(74.3%)患者根据 mFFC 评估为虚弱和非虚弱。单因素分析显示,年龄、Charlson 合并症指数和虚弱(mFFC)(单因素 OR 13.00,95%CI 2.21-76.63, < 0.01)与 1 年内丧失功能独立性显著相关。然而,与 mFFC 相比,mFI-11 评估的虚弱相关性较弱(单因素 OR 4.42,95%CI 0.84-23.12, = 0.06)。多因素分析显示,仅术前虚弱(mFFC)仍具有统计学意义(OR 15.63,95%CI 2.12-111.11, < 0.01)。
mFFC 可用于筛选接受急诊腹部手术的老年患者的虚弱情况,是 1 年内丧失功能独立性的预测因素。在与患者及其护理人员进行围手术期讨论时,将丧失功能独立性的风险纳入其中对于以患者为中心的急诊外科护理非常重要。早期识别这一高危人群有助于制定出院计划,并应考虑为其提供优先的出院后支持。