1Service de Pédiatrie-Urgences, Hôpital Louis-Mourier, APHP, 178 rue des Renouillers, 92700 Colombes, France.
2Paediatric Infectious Diseases Research Group, Institute of Infection and Immunity, St George's, University of London, London, UK.
Antimicrob Resist Infect Control. 2019 Dec 30;8:207. doi: 10.1186/s13756-019-0673-5. eCollection 2019.
Despite a high mortality rate in childhood, there is limited evidence on the causes and outcomes of paediatric bloodstream infections from low- and middle-income countries (LMICs). We conducted a systematic review and meta-analysis to characterize the bacterial causes of paediatric bloodstream infections in LMICs and their resistance profile.
We searched Pubmed and Embase databases between January 1st 1990 and October 30th 2019, combining MeSH and free-text terms for "sepsis" and "low-middle-income countries" in children. Two reviewers screened articles and performed data extraction to identify studies investigating children (1 month-18 years), with at least one blood culture. The main outcomes of interests were the rate of positive blood cultures, the distribution of bacterial pathogens, the resistance patterns and the case-fatality rate. The proportions obtained from each study were pooled using the Freeman-Tukey double arcsine transformation, and a random-effect meta-analysis model was used.
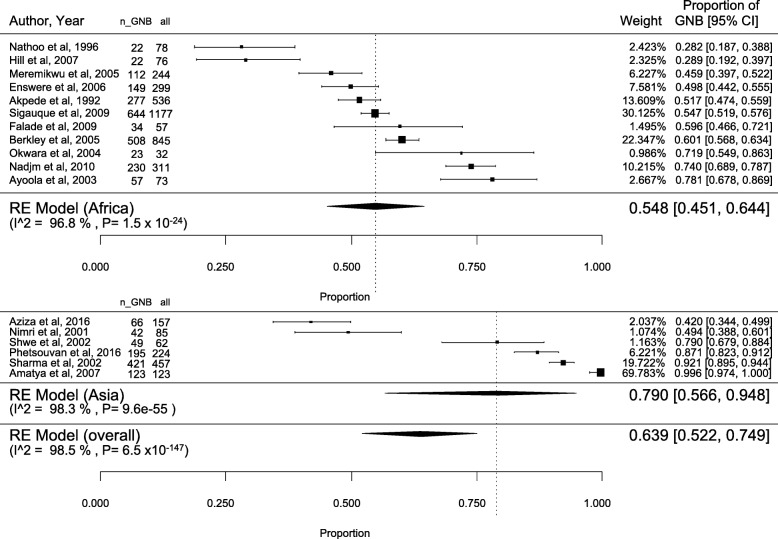
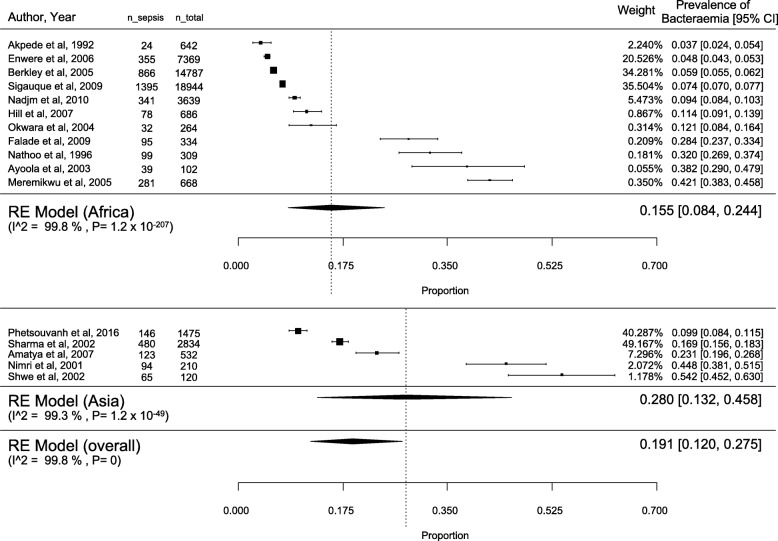
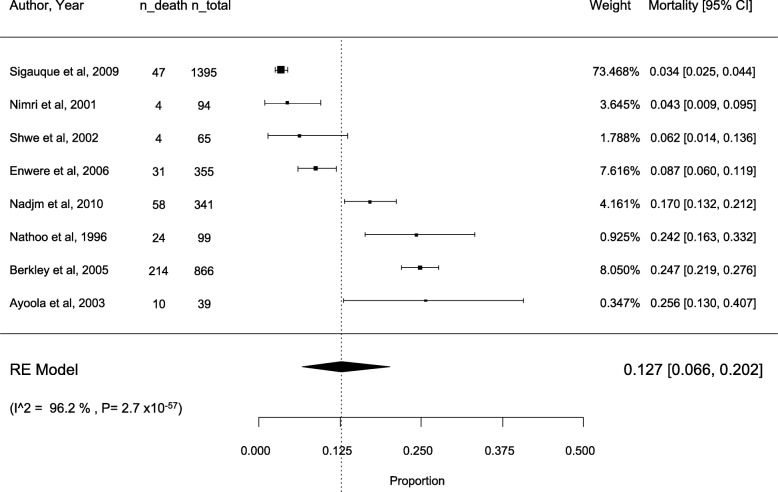
We identified 2403 eligible studies, 17 were included in the final review including 52,915 children (11 in Africa and 6 in Asia). The overall percentage of positive blood culture was 19.1% [95% CI: 12.0-27.5%]; 15.5% [8.4-24.4%] in Africa and 28.0% [13.2-45.8%] in Asia. A total of 4836 bacterial isolates were included in the studies; 2974 were Gram-negative (63.9% [52.2-74.9]) and 1858 were Gram-positive (35.8% [24.9-47.5]). In Asia, typhi (26.2%) was the most commonly isolated pathogen, followed by (7.7%) whereas in Africa, (17.8%) and (16.8%) were predominant followed by (10.7%). was more likely resistant to methicillin in Africa (29.5% vs. 7.9%), whereas was more frequently resistant to third-generation cephalosporins (31.2% vs. 21.2%), amikacin (29.6% vs. 0%) and ciprofloxacin (36.7% vs. 0%) in Asia. The overall estimate for case-fatality rate among 8 studies was 12.7% [6.6-20.2%]. Underlying conditions, such as malnutrition or HIV infection were assessed as a factor associated with bacteraemia in 4 studies each.
We observed a marked variation in pathogen distribution and their resistance profiles between Asia and Africa. Very limited data is available on underlying risk factors for bacteraemia, patterns of treatment of multidrug-resistant infections and predictors of adverse outcomes.
尽管儿童的死亡率很高,但来自中低收入国家(LMICs)的儿科菌血症的病因和结果的证据有限。我们进行了系统评价和荟萃分析,以描述 LMICs 中儿科菌血症的细菌病因及其耐药谱。
我们在 1990 年 1 月 1 日至 2019 年 10 月 30 日期间在 Pubmed 和 Embase 数据库中进行了搜索,结合了“败血症”和“中低收入国家”的 MeSH 和自由文本术语,用于儿童。两名审查员筛选文章并进行数据提取,以确定至少有一项血培养的研究。主要关注的结果是阳性血培养的比率、细菌病原体的分布、耐药模式和病死率。从每项研究中获得的比例使用 Freeman-Tukey 双反正弦变换进行汇总,并使用随机效应荟萃分析模型。
我们确定了 2403 项合格的研究,其中 17 项最终审查包括 52915 名儿童(11 项在非洲,6 项在亚洲)。阳性血培养的总体百分比为 19.1%[95%CI:12.0-27.5%];非洲为 15.5%[8.4-24.4%],亚洲为 28.0%[13.2-45.8%]。共有 4836 株细菌分离株纳入研究;革兰氏阴性菌 2974 株(63.9%[52.2-74.9%]),革兰氏阳性菌 1858 株(35.8%[24.9-47.5%])。在亚洲, 最常分离到的病原体是 (26.2%),其次是 (7.7%),而在非洲, (17.8%)和 (16.8%)是主要病原体,其次是 (10.7%)。在非洲, 对甲氧西林的耐药性更可能(29.5%比 7.9%),而 对第三代头孢菌素(31.2%比 21.2%)、阿米卡星(29.6%比 0%)和环丙沙星(36.7%比 0%)的耐药性更常见亚洲。8 项研究中病死率的总体估计为 12.7%[6.6-20.2%]。4 项研究评估了营养不良或 HIV 感染等潜在疾病作为菌血症相关因素,4 项研究评估了潜在疾病作为菌血症相关因素。
我们观察到亚洲和非洲之间病原体分布和耐药谱存在明显差异。关于菌血症的潜在危险因素、多药耐药感染的治疗模式和不良结局预测因素的数据非常有限。