Division of Maternal Fetal Medicine, Department of Gynecology and Obstetrics, Johns Hopkins University School of Medicine, Baltimore, MD.
Department of Obstetrics and Gynecology, University of Southern California School of Medicine, Los Angeles, CA.
J Acquir Immune Defic Syndr. 2020 Apr 1;83(4):373-380. doi: 10.1097/QAI.0000000000002261.
This study aims to evaluate the pharmacokinetics of an increased dose of darunavir (800 mg twice daily) with 100 mg ritonavir during pregnancy and postpartum.
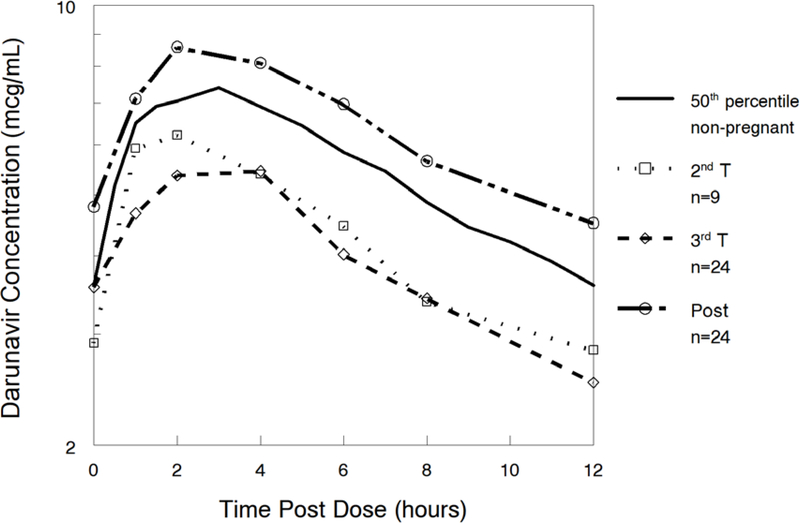
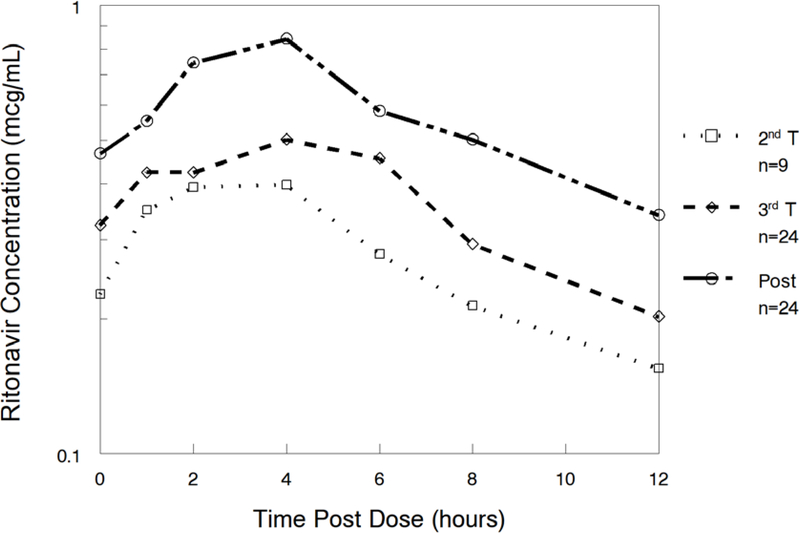
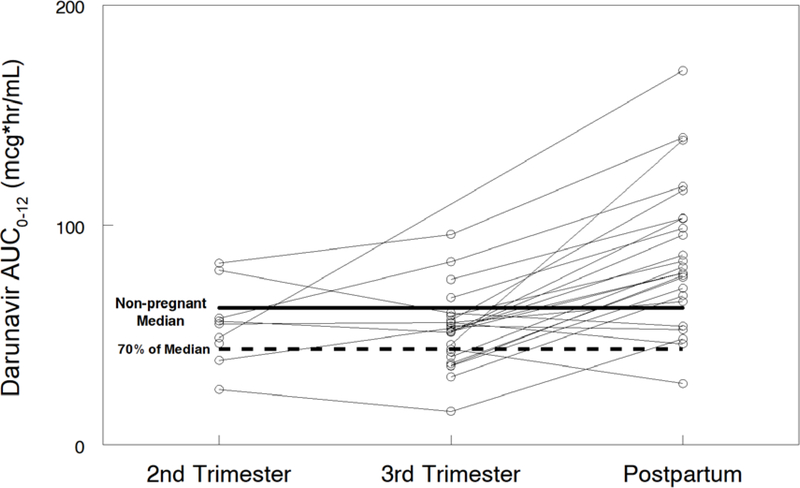
Darunavir (DRV) and ritonavir (RTV; r) intensive pharmacokinetic evaluations were performed at steady state during the second and third trimesters of pregnancy (DRV/r 800/100 mg bid) and 2-3 weeks postpartum (DRV/r 600/100 mg twice daily). Plasma concentrations of darunavir and ritonavir were measured using high-performance liquid chromatography. Target darunavir area under the concentration time curve (AUC) was >70% (43.6 μg × h/mL) of median AUC (62.3 μg × h/mL) in nonpregnant adults on twice daily darunavir-ritonavir 600/100 mg.
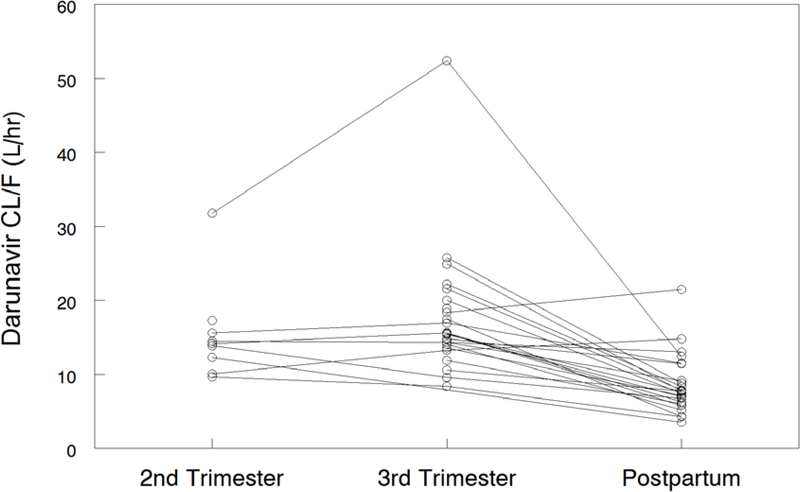
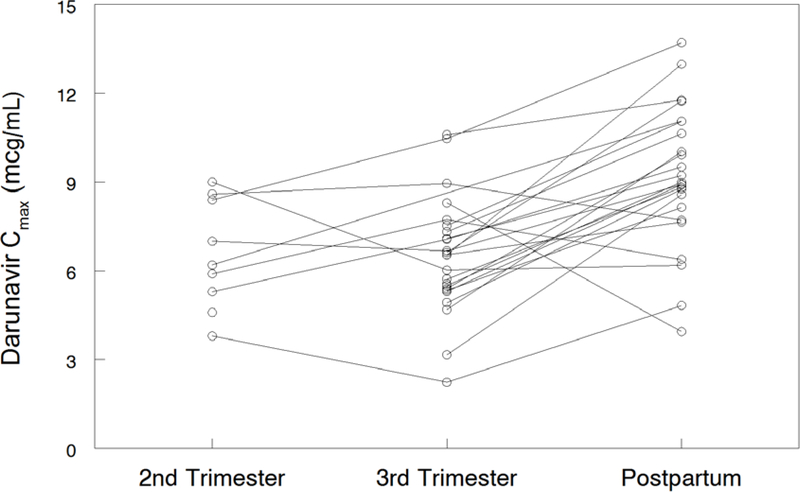
Twenty-four women were included in the analysis. Darunavir AUC0-12 was lower with the increased dose during the second {[geometric mean ratio (GMR) of 0.62 (IQR 0.44-0.88); P = 0.055]} and third trimesters [GMR 0.64 (IQR 0.55-0.73); P = <0.001] compared with postpartum. Darunavir apparent clearance was higher during the second [GMR 1.77 (IQR 1.24-2.51); P = 0.039] and third trimesters [GMR 2.01 (IQR 1.17-2.35); P = <0.001] compared with postpartum. Similarly, ritonavir AUC0-12 was lower during the third trimester [GMR 0.65 (IQR 0.52-0.82); P = 0.007] compared with postpartum, whereas its apparent clearance was higher during the third trimester [GMR 1.53 (IQR 1.22-1.92); P = 0.008] compared with postpartum. No major drug-related safety concerns were noted.
Increasing darunavir dose to 800 mg BID failed to significantly increase darunavir exposure compared with 600 mg BID. Other strategies, such as increasing the ritonavir dose should be investigated.
本研究旨在评估孕期和产后应用利托那韦增强剂量(800mg,每日 2 次)的达鲁那韦(800mg,每日 2 次)的药代动力学。
在妊娠第二和第三个三个月(DRV/r 800/100mg bid)和产后 2-3 周(DRV/r 600/100mg bid)时,对达鲁那韦(DRV)和利托那韦(RTV;r)进行强化药代动力学评估。采用高效液相色谱法测定达鲁那韦和利托那韦的血浆浓度。在接受每日两次 600/100mg 达鲁那韦-利托那韦治疗的非妊娠成年人中,目标达鲁那韦 AUC(43.6μg×h/mL)>中位数 AUC(62.3μg×h/mL)的 70%。
24 名女性纳入分析。与产后相比,在妊娠第二[几何均数比(GMR)为 0.62(IQR 0.44-0.88);P=0.055]和第三个三个月[GMR 0.64(IQR 0.55-0.73);P<0.001]时,增加剂量的达鲁那韦 AUC0-12 较低。与产后相比,在妊娠第二[GMR 1.77(IQR 1.24-2.51);P=0.039]和第三个三个月[GMR 2.01(IQR 1.17-2.35);P<0.001]时,达鲁那韦的表观清除率较高。同样,与产后相比,在妊娠第三个三个月时,利托那韦 AUC0-12 较低[GMR 0.65(IQR 0.52-0.82);P=0.007],而其表观清除率在妊娠第三个三个月较高[GMR 1.53(IQR 1.22-1.92);P=0.008]。未观察到与药物相关的重大安全性问题。
与每日 600mg 相比,增加达鲁那韦剂量至 800mg 每日 2 次并未显著增加达鲁那韦的暴露量。应研究其他策略,例如增加利托那韦剂量。