Cosansu Kahraman, Ureyen Cagin Mustafa, Vatan Mehmet Bulent, Agac Mustafa Tarik, Kilic Harun, Akdemir Ramazan
Department of Cardiology, Sakarya University Education and Research Hospital, Sakarya, Turkey.
Department of Cardiology, Antalya Education and Research Hospital, Antalya, Turkey.
Postepy Kardiol Interwencyjnej. 2019;15(4):404-411. doi: 10.5114/aic.2019.90214. Epub 2019 Dec 8.
Direct stenting (DS) is associated with improved markers of reperfusion during primary percutaneous coronary intervention (PPCI) for ST-elevation myocardial infarction (STEMI). However, data evaluating its impact in small vessel coronary artery disease (CAD) are lacking.
To compare DS and conventional stenting (CS) for small vessel CAD on clinical outcomes of patients with STEMI undergoing PPCI.
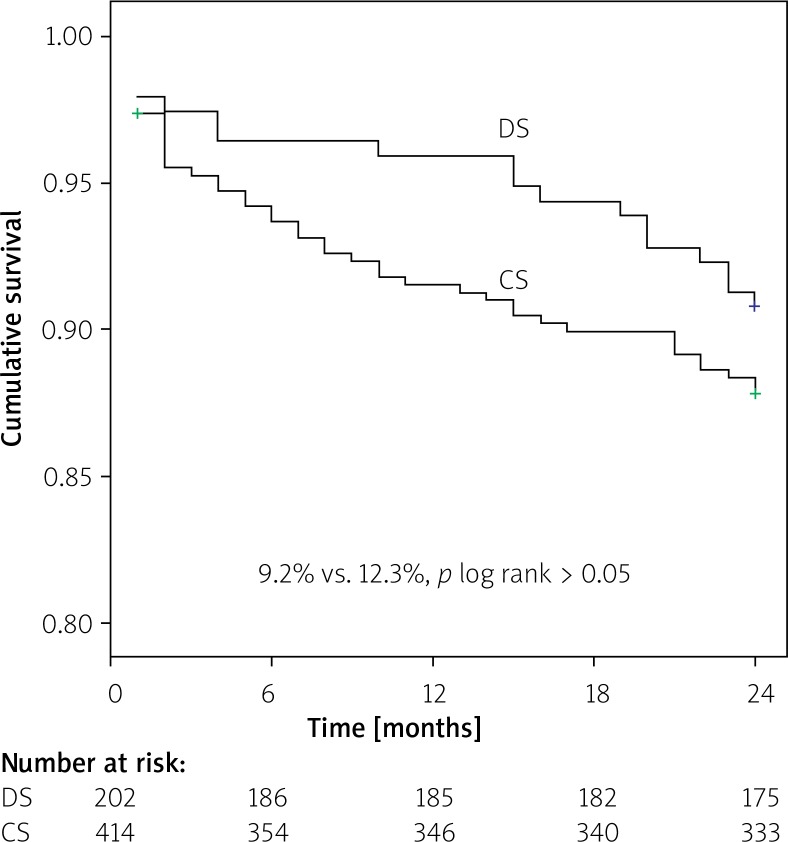
A cohort of 616 STEMI patients treated with DS (202 patients) or CS (414 patients) in small vessel (≤ 2.75 mm) lesions was retrospectively analyzed. The primary endpoint was to compare the occurrence of major adverse cardiac events (MACE) between groups during 2-year follow-up. The secondary end points included in-hospital target lesion revascularization (TLR) and in-hospital death.
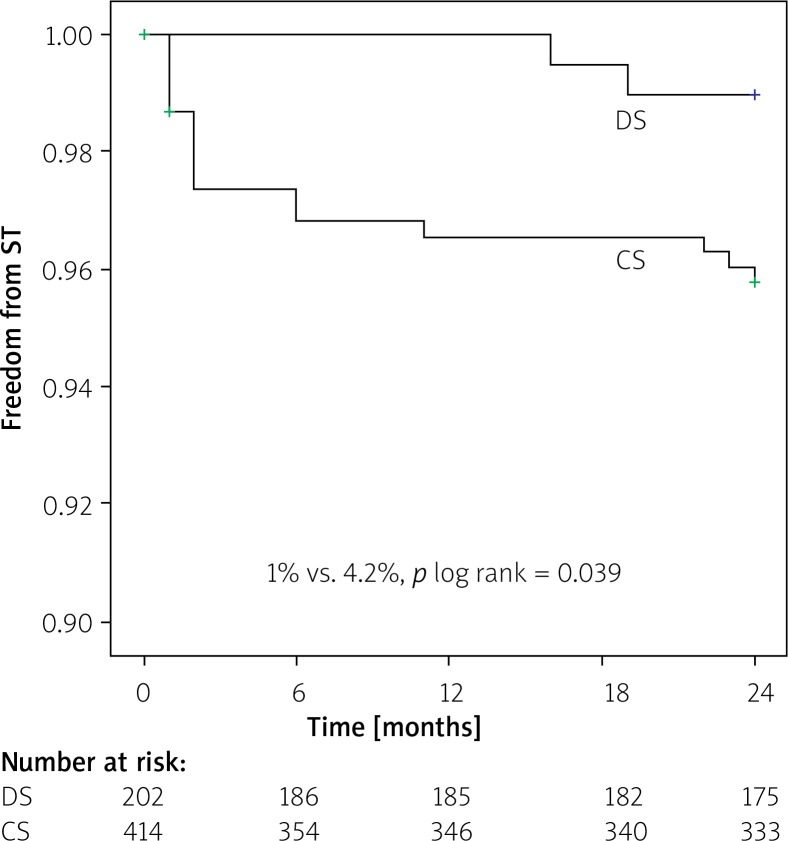
The primary end-point, MACEs, occurred in 9.2% in the DS group and 12.3% in the CS group ( > 0.05). The rates of TLR, myocardial infarction (MI) and target vessel revascularization (TVR) were not significantly different between groups ( > 0.05). The stent thrombosis (ST) rate was significantly lower in the DS group (1.0% vs. 4.2%, = 0.04) at 2 years. However, DS was not found to be an independent predictor of ST in multivariate analysis. There were no significant differences in in-hospital rates of death and TLR. The DS compared to CS resulted in greater rates of postprocedural TIMI grade 3 flow, and lower risk of edge dissection. The procedure time, radiation exposure and contrast administration were found to be significantly lower in the DS group.
In selected patients with STEMI undergoing PPCI for small vessel CAD, DS is not only safe and feasible but also reduces ST rates, contrast load, and procedural and radiation exposure time.
在ST段抬高型心肌梗死(STEMI)的直接经皮冠状动脉介入治疗(PPCI)期间,直接支架置入术(DS)与再灌注指标改善相关。然而,评估其在小血管冠状动脉疾病(CAD)中影响的数据尚缺乏。
比较DS和传统支架置入术(CS)在接受PPCI的STEMI患者小血管CAD临床结局方面的差异。
回顾性分析616例在小血管(≤2.75mm)病变中接受DS(202例患者)或CS(414例患者)治疗的STEMI患者队列。主要终点是比较两组在2年随访期间主要不良心脏事件(MACE)的发生率。次要终点包括院内靶病变血运重建(TLR)和院内死亡。
主要终点MACE在DS组发生率为9.2%,CS组为12.3%(P>0.05)。两组间TLR、心肌梗死(MI)和靶血管血运重建(TVR)率无显著差异(P>0.05)。2年时DS组支架血栓形成(ST)率显著更低(1.0%对4.2%,P=0.04)。然而,多变量分析中未发现DS是ST的独立预测因素。院内死亡和TLR率无显著差异。与CS相比,DS导致术后TIMI 3级血流发生率更高,边缘夹层风险更低。发现DS组手术时间、辐射暴露和造影剂用量显著更低。
在选择接受PPCI治疗小血管CAD的STEMI患者中,DS不仅安全可行,而且可降低ST率、造影剂负荷以及手术和辐射暴露时间。